Yeah, the fact that this doesn't even need a freezer is great news.
The fact that we have three highly effective vaccines in such a short period is amazing and between them we might stand a chance of making and distributing them at the scale necessary to get things under some kind of control by August.
The safety concerns cannot be resolved yet. Effective - yes. Safe? We won’t know for a while.
Pandemrix, a flu vaccine, caused a notable uptick in narcolepsy in Sweden, Finland and likely the UK. This was not (and could not) be seen in smaller trial populations.
It is not a given that any of the covid vaccines is safe enough. Historically, two cases of rushed vaccines (cutter polio and Gullah barre) were worse than the disease - and these were for diseases worse than covid. Those were 50-60 years ago. Pandemrix was 10-20. I’m not sure we’re that much better on safety now to rush vaccines.
If the association between Pandemrix and narcolepsy is because it caused narcolepsy (as with Guillain-Barré it's also plausible the problem is that this is an auto-immune problem and so the vaccine wasn't actually the problem it just highlighted a problem you already had) then the incidence rate was estimated at like 18k patients per case.
So if you give the entire US population a vaccine like that, less than twenty thousand of them develop narcolepsy. As a reminder a quarter million of them already died from COVID-19 and more are dying every day - not to mention the tens of thousands whose cause of death isn't listed as COVID-19 but would not be dead if not for an ongoing pandemic.
Cutter screwed up. No amount of prior safety testing can fix that. Their Polio vaccine had Polio virus in it (to be clear: The traditional Oral Polio Vaccine is supposed to have a "live" virus in it, but the injected vaccine Cutter were selling is not). Obviously nobody is going to test "What happens if we inject children with the Polio virus" because the answer is "Some of them get Polio. Duh" and so no test could have prevented Cutter from screwing up.
I have no idea what you meant by "Gullah barre" the Google results I get are all about Guillain-Barré syndrome, which I mentioned above. Guillain-Barré is not a vaccine, it's a weird auto-immune disorder, and arguably even where it's listed as very rare side effect of a vaccine, that's misleading because it's also a side effect from getting viral infection, so if you avoid vaccination but do get the virus you may get GBS as a result anyway. The human immune system is pretty inscrutable.
> less than twenty thousand of them develop narcolepsy. As a reminder a quarter million of them already died from COVID-19 and more are dying every day
I assume the concern is that an unknown unknown means it could cause/trigger/amplify some other disease/condition that may be comparable/worse than the problem it solves.
Cause/effect and morals are hard. Add to the mix a general statistical innumeracy, and some general suspicion about authorities, and it makes it really hard for the general populace to actually weigh the two different options.
I don't think we should dismiss these concerns as just stuff for nutjobs. I've seen otherwise reasonable people having trouble making up their minds about that.
The association in Sweden is strong enough to say “it does”.
And yes, the mechanism is likely that Pandemrix activated a predisposition. But it was not activated in statistically equivalent kids who did not get Pandemrix.
Why is it so hard to acknowledge that not all vaccines are perfect, and that there’s a risk involved? I am not avtivax. I am pro vaccination. I am anti religious “a vaccine can never be bad” thinking which seem to be prevalent among otherwise rational scientific people.
covid risk varies wildly depending on socioeconomic factors. Educated, WFH, small family, stable or low IRL social interaction: pretty low risk. Low-education, multiple in-person jobs, lots of casual social interaction, large family: very high risk. We've seen it very starkly in England. When entire communities are being ravaged by exponentially-growing transmission, it's hard to argue that a vaccine might be worse, because the chances are really minimal.
> Historically, two cases of rushed vaccines (cutter polio and Gullah barre) were worse than the disease - and these were for diseases worse than covid.
This is just patently untrue.
The Cutter Incidence gave patients Polio due to an improperly activated virus. While this is bad, it could not be worse than the disease itself - since it is the disease itself, no worse, no less.
Regarding risk of Gullain-Barre syndrome due to vaccination, Wikipedia has this to say: "In fact, natural influenza infection is a stronger risk factor for the development of GBS than is influenza vaccination and getting the vaccination does reduce the risk of GBS overall by lowering the risk of catching influenza." So here I also find it hard to believe the vaccine would be worse than the disease,
I'm also sceptical of the claim that Polio or the 1976 Swine Flu would unambiguously be worse than Covid19. 70% of Polio case have no symptoms, and less than 0.5% cause permanent injury, according to Wikipedia. The 1976 Swine Flu outbreak seems to have caused a few hundred cases and only one death.
No, the cutter incidence was worse than the disease, because the activated virus was injected into a population, whereas naturally only a tiny part would be exposed at the same level, and the rest would be exposed at a much lower level - that would give them immunity but not disease.
Cutter was, most definitely, much worse than the disease if you look at it from a population perspective.
The 1976 Guilian barre was at least comparable to the flu it was supposed to stop, if not worse. According to https://en.m.wikipedia.org/wiki/1976_swine_flu_outbreak, the disease caused one death and 13 hospitalizations, and an uptick of Giullan barre reports - a disease that more often than not requires hospitalization and sometimes death. I can assure you it caused more than 13 hospitalizations, and - having known two GBS people who made a full recovery - a very long and painful months long process. So, at 50,000,000 immunized - a 1 in 1,000,000 would still be worse than the flu.
I am not anti vax even if HN constantly seems to interpret my comments as such.
I am vaccinated, so are my kids. But whenever I mention that immunizations have risks, I’m treated like a heretic.
Everyone is assuming something like cutter cannot happen again. This is a religious assumption, not a scientific one.
> No, the cutter incidence was worse than the disease, because the activated virus was injected into a population, whereas naturally only a tiny part would be exposed at the same level, and the rest would be exposed at a much lower level - that would give them immunity but not disease.
This is a more reasonable assessment, but it is still patently false. According to Wikipedia, 0.04% vaccinations resulted in paralysis in the Cutter Incident, compared to 0.1-0.5% of wild type polio. So the vaccine was 2-10x safer than wild polio. Without vaccinations, virtually all children were infected with polio virus early in life [1], so being administered the defective vaccine was still a lot better than taking a chance with the real disease.
Of course, you are correct regarding the 1976 flu outbreak. If you administer something to a large segment of the healthy population, even a small risk of side-effects will add upp to a large number of cases. If the disease itself turns out to be very rare, as was the case with the flu outbreak, the vaccine itself could cause more damage than the disease even if the disease is much worse.
However, this is clearly not applicable Covid-19, which we already know is spreading very fast and will need to infect a large number of the population before herd immunity is achieved. The situations are simply not comparable at all – even the vaccine from the 1976 flu outbreak would be less risky than the odds of being infected with a serious case of Covid 19 (of which the long term effects are also unknown, to be clear).
> But whenever I mention that immunizations have risks, I’m treated like a heretic.
Mainstream media, healthcare professionals and social media are all worried about the risks of a rushed vaccine. I literally see articles and hear conversations about this several times a month. Nobody is denying that large scale vaccinations have risks.
I'm not criticizing you because I'm against being cautious of vaccination risks. The criticism is that you are spreading false facts and misleading analysis that grossly mischaracterise what the risks of vaccinations really are, both presently and historically.
"Some vaccines can have rare but serious side effects" is a perfectly alright statement. But "Historically, two cases of rushed vaccines (cutter polio and Gullah barre) were worse than the disease - and these were for diseases worse than covid" is just not. Some of it is false and the comparison to Covid19 is misleading.
> According to Wikipedia, 0.04% vaccinations resulted in paralysis in the Cutter Incident, compared to 0.1-0.5% of wild type polio.
From https://en.wikipedia.org/wiki/Polio_vaccine#1950%E2%80%93195... : "The Cutter vaccine had been used in vaccinating 200,000 children in the western and midwestern United States.[76] Later investigations showed that the Cutter vaccine had caused 40,000 cases of polio, killing 10.[76]". So, 20% incidence; mentions 250 "paralytic illness", so 0.125% paralysis (no idea where you took the 0.04% - it does not appear in the Wikipedia text).
From https://en.wikipedia.org/wiki/Polio#Paralytic_polio : "In children, nonparalytic meningitis is the most likely consequence of CNS involvement, and paralysis occurs in only one in 1000 cases." ; So, for children, the incidence of paralysis is 0.1%
Who got the cutter vaccine? Mostly children. See e.g. from https://www.washingtonpost.com/history/2020/04/14/cutter-pol... "By April 30, within forty-eight hours of the recall,” Offit wrote. “Cutter’s vaccine had paralyzed or killed twenty-five children: fourteen in California, seven in Idaho, two in Washington, one in Illinois, and one in Colorado."
So, I just tried to check your numbers, and I couldn't; Could you post references?
But I also wanted to check my memory, and Wikpedia seems to agree with me, Go on, please do check my quotes.
still patently false. pfft. Perhaps false under some assumptions, definitely not "patently false".
You are almost certainly using the wrong numbers. According to https://en.wikipedia.org/wiki/Cutter_Laboratories#Cutter_inc... and https://www.nejm.org/doi/full/10.1056/NEJMp048180, the faulty production applied to 120.000 doses of vaccine, which lead to 56 cases of paralysis (0.046%) among vaccinated children. These sources further mention "the exposures led to an epidemic of polio in the families and communities of the affected children, resulting in a further 113 people paralyzed and 5 deaths", which tells me that your number of 250 probably includes cases caused by such transmission. This is of course reasonable when discussing the total damage caused by the vaccine, but this number can not be compared to the incidence of paralysis for a single infection, as you do.
You would also have to include further transmissions caused by wild polio if you would like to make such a comparison.
> still patently false. pfft. Perhaps false under some assumptions, definitely not "patently false".
Even with your own calculation, which is inflated by also including transmission within the community for the vaccine but not for wild polio, the vaccine was very much comparable to wild polio (0.125% versus approx. 0.1%). Without vaccination, polio would usually infect virtually all children. So even with your own inflated assumptions it's false that the vaccine was worse than polio.
> You are almost certainly using the wrong numbers
Take them with wikipedia, not me. I will note, that Wikipedia talks about both Cutter and Wyeth having problems, so it is possible the numbers are a sum of wyeth+cutter which would be compatible with your numbers being cutter only, but in the context of safety vs. polio wouldn't matter.
> You would also have to include further transmissions caused by wild polio if you would like to make such a comparison.
All wild polio numbers include those numbers by default - there actually is no way to get them otherwise, I guess you are saying "you should probably debase by more than 200,000 because of secondary infections". I don't know how to do that, exactly, but it will likely still be similar.
> Even with your own calculation, which is inflated by also including transmission within the community for the vaccine but not for wild polio, the vaccine was very much comparable to wild polio (0.125% versus approx. 0.1%).
With this calculation, the vaccine was 25% worse than the wild type. No error bars, but, that's easily worse, even much worse.
> So under which assumptions would it not be false?
How kind of you to drop "patently". If you didn't mean "patently" false earlier, why did you use that word? twice?
From[0]: "Patently: in a way that is so obvious that no one could disagree.". It's nice of you to finally bring sources, but even these sources don't make it "patently" false, given that they disagree with the sources I gave (which, I concede, reference more than just the safety of the Cutter incident which I originally mentioned, but which are definitely the subject matter under discussion)
> Take them with wikipedia, not me. I will note, that Wikipedia talks about both Cutter and Wyeth having problems, so it is possible the numbers are a sum of wyeth+cutter which would be compatible with your numbers being cutter only, but in the context of safety vs. polio wouldn't matter.
Wikipedia is not wrong, but you are using their numbers wrong. Your source is talking about the total number paralysis cases that occurred as a result of the vaccine ("250 cases of paralytic illness had occurred"). This includes secondary infections. If you follow the sources listed on Wikipedia page you reference, you will find two sources: my source [1], and [2] (via [3]), both which declare around 60 cases of paralysis in vaccinated persons, and then a larger number (in the order of 200) of total cases. The numbers you reference are referring to only the Cutter polio vaccine, by the way.
And you cannot use the total number of cases in the comparison that you did.
> All wild polio numbers include those numbers by default - there actually is no way to get them otherwise, I guess you are saying "you should probably debase by more than 200,000 because of secondary infections". I don't know how to do that, exactly, but it will likely still be similar.
If by debase you mean divide, then yes: you would need to divide by more than 200,000.
Your number is {how likely am I to get paralysed by the vaccine polio + how likely am I to cause further paralysis via secondary infection chain}, and you are comparing it to simply {how likely am I to get paralysed by the wild polio}. The first number is inflated a lot by the addition of secondary infections.
The numbers are not at all likely to be similar. As you can see in my (and your) sources, secondary infections accounted for more than double the number of paralysis cases, and therefore there it is likely a lot more people got sick via the secondary infections than the number people who was vaccinated. This causes the big discrepancy between our numbers.
Wild polio causes secondary infections as well, but this is not included in the number you are using for comparison, since it only includes the individual risk.
> With this calculation, the vaccine was 25% worse than the wild type. No error bars, but, that's easily worse, even much worse.
But the lack of error bars means that the calculation is meaningless.
You are assuming that "one in 1000 cases" means exactly one case per 1000 cases, and translate this to 0.100% with three decimals of accuracy.
It is clear from context that "one in 1000" is a rounded number for convenience, and they could very well have runded up from 0.8 or down from 1.4. You simply cannot conclude that the vaccine was 25% worse from your data. But we can conclude that they were in some way similar under your false assumptions, as they both would round to 1.
If you want to conclude anything else except "they are both around 0.1%", you would have to find a source that specifies at least 1 decimal of accuracy in the number incidents per 1000 cases.
Of course, this does not really matter, since you would still be comparing the wrong numbers.
Your argument here is "It's ambiguous and inconclusive when using clearly wrong assumptions that inflate the difference". Taking that argument into consideration, I'm still willing to confidently call it patently false.
Although I agree that I should not have said "Even with your own inflated assumptions it's false that the vaccine was worse than polio." What I meant was "Even your own inflated assumptions does not support that the vaccine was worse than polio", but I clearly worded it badly.
> How kind of you to drop "patently". If you didn't mean "patently" false earlier, why did you use that word? twice?
I meant it when I used it, and my question had a purpose. If you cannot give any reasonable assumptions where it wouldn't be false (which you haven't been able to do), then it would be patently false to me. The reason it does not seem patently false to you is because you have several misunderstandings in your reasoning and your reading of the sources. But I'm not really interested in discussing this terminology further.
> given that they disagree with the sources I gave
They don't. As I said, you are simply misreading your sources.
But seriously, even if you would manage to find some source which would refute my sources and back up your original claims, I have a bigger point to make now:
During this discussion, you have made numerous mistakes in many posts, beyond my criticism of your faulty reasoning:
(1) Mathematical mistakes
(2) Misreadings of the sources
(3) Inability to clear up ambiguities by looking at the referenced source or secondary sources
Even if by some happenstance you would happen to be right (even a broken clock, etc), you clearly are not confident enough doing this kind of analysis to be lecturing people about the specifics of vaccination risks. You are just as likely to mislead yourself and others as you are to educate.
Of course, this probably won't stop you, since you are not likely to respect my opinion. But hopefully it will still be in the back of your mind next time you approach this topic.
Thank you for your thoughtful answer. I pointed the lack of error bars myself, as well as mentioned that I don’t know what other number to divide by, as you noted. I am not trying to be intellectually dishonest.
And I may agree with your analysis - on phone now, can’t really do the reading.
However, we have two sources you claim are only for the cutter incident, whee one quotes 200,000 doses and another 120,000; as you note, the 1/1000 might well be 0.8 or 1.3 in 1000; it may be false but it is definitely bot “patently false”.
On the same note, it’s the internet, and for all you know I am a dog, but I have saved a family members from years of
agony and wrong treatments due to wrong diagnosis after being told “it is patently obvious” that my analysis was wrong. And I have apology letters from department heads at two of the world’s highest ranked hospitals after it turned out I was right and they were wrong.
And you know what? I’m quite sure I probably had a few mathematical errors along the way back then as well. But what they thought was two orders of magnitude more probable evidence towards one direction, turned out to be higher probability in the other (by less than an order of magnitude) and turned out to be what the thought was improbable beyond consideration. (And, I found a few mathematical errors in a three peer reviewed papers they were relying on)
I take issue with people who claim “patently obvious” about things which have about factor of 2 or so (if I take your numbers) without error bars (120000-200000 is a large difference) and without supplying sources, which you didn’t bother until I did.
(And I may not have time to delve into this further - this is merely of historical interest to me, not life and death like that other event).
Also, you may notice this sub thread is basically the only one that actually discusses numbers, others use arbitrary determinations like “most people’s living memory” to discard concerns. Despite advocating vaccines myself, I have a problem with religious zealotry around vaccines, which is what most pro-vaccine people practice - I have a child who could not get vaccines for medical reasons for many years, and I have to explain that, no, vaccines are not perfectly safe on an individual basis, and have not historically been perfectly safe on a population basis (Swedish Pandemrix), even though on a net population basis they are a net positive.
On the one hand I tend to agree, and all my expectations for this vaccine are positive. The medical industry tends to be paranoid to a level that exceeds rationality and even if they dropped their standards for this that should only get them down to "conservative and rather safe" levels of caution.
On the other, a cursory search says the current record for fastest developed vaccine was mumps at 4 years. So this is a vaccine setting new milestones, and there is a risk that not all of them will be positive. I'd rather be a little late to be vaccinated than a little early, especially being in a lower risk demographic.
I'm not an expert by any means, but I do know that a lot of the speed comes from moving along the CHEAP-FAST side of the CHEAP-FAST-SAFE triangle, without necessarily changing anything on the FAST-SAFE axis. In particular, governments paid for the companies to start producing enough vaccines for phase 3 trials before phase 1 was complete, while normally drug companies would wait for phase 1 to be completed before preparing for phase 2 for economic reasons.
BiondVax recently finished their phase 3 trial of a universal flu vaccine. It was 15 years in the making. Science was (still is solid). Phase 3 took two years to account for ADE and other safety issues.
At the 1-year mark, everything looked perfect. At the towo years mark (original endpoint) the conclusion was that while it was safe, it offered statistically insignificant protection.
Properly designed tests need those 2 years, at the very least. The “SAFE” confidence axis was compromised. Whether or nit it is justified is what we’re discussing here.
I'm very pro-vaccine, and not disagreeing with your conclusions, but your logic leaves out the consideration that the natural risk also depends on catching the disease, whereas the vaccine is administered systematically.
I have had Guillain-Barre Syndrome (not due to a vaccine). No matter what, I still always get my vaccines and make sure that I am up to date and never late on any of them.
Sure, having Guillain-Barre is scary, but it is something that you can make a full recovery from.
It is never an excuse NOT to get a vaccine, unless you actually know that you got Guillain-Barre Syndrome from a vaccine. That is a discussion between that particular patient and their neuromuscular neurologist. In that case, you do not get the flu vaccine any longer because it can cause you to experience Guillain-Barre Syndrome again.
But, this really is an isolated situation that can be categorized as very rare and the general public should always get their vaccines.
If you catch the flu, it can absolutely trigger Guillain-Barre Syndrome, and would be far more likely to trigger Guillain-Barre Syndrome than the flu vaccine itself. If you get the flu and had the flu vaccination, it typically makes the flu illness less worse, making you less likely to get something like Guillain-Barre Syndrome.
There are lots of infectious agents that can trigger Guillain-Barre Syndrome, so it is wise to get your vaccines to prevent them as much as possible. They prevent serious infections, at minimum, which would help prevent Guillain-Barre Syndrome.
I also have the long term variant of Guillain-Barre Syndrome, known as Chronic Inflammatory Demyelinating Polyneuropathy, which is in pharmaceutical remission due to me taking subcutaneous immunoglobulin twice a week for 3 hours each time.
What I am saying is that while all of this sounds rare and devastating, it’s treatable. Not only that, you’re more likely to get Guillain-Barre Syndrome from a bad case of the flu than from a flu shot.
“Even at this stage, it does not appear that narcolepsy following vaccination against pandemic influenza is a general worldwide phenomenon, as no excess of narcolepsy has been reported from several other European states where Pandemrix was used, or from Canada where a pandemic vaccine similar to pandemrix was used. This complicates interpretation of the findings in Finland and Sweden. It seems likely that some as yet unidentified additional factor was operating in Sweden and Finland. The findings from the VAESCO project and further investigations in Finland and Sweden, may help clarify the determinants of any increased risk of narcolepsy, which currently appears to be restricted to the months following vaccination and by age group and country.”
What’s certainly true that for some effects to be observable, millions have to be vaccinated first.
“In total, the GSK shot was given to more than 30 million people in 47 countries during the 2009-2010 H1N1 swine flu pandemic.”
“Independent teams of scientists have published peer-reviewed studies from Sweden, Finland and Ireland showing the risk of developing narcolepsy after the 2009-2010 immunization campaign was between seven and 13 times higher for children who had Pandemrix than for their unvaccinated peers.”
“Europe’s drugs regulator has ruled Pandemrix should no longer be used in people aged under 20.”
> Pandemrix, a flu vaccine, caused a notable uptick in narcolepsy in Sweden, Finland and likely the UK.
"The increased risk of narcolepsy due to vaccination was 1 in 18400 or 0.005%."[1] Considering the fatality and long term disability rate of Covid, and the way testing and safety protocols are done for vaccines, I don't really see how there could be an unknown and unseen risk that would outweigh the risk of contracting Covid.
The risk of death in kids without underlying diseases is is approximately 0. It is not clear that giving (e.g. in the US) 30,000 of these kids narcolepsy is reasonable.
As far as I know, none of the COVID19 vaccines have been tested on children under 12 or are currently planned on being given to children.
Additionally, it's not as if the average vaccine has a 0.005% chance of giving you narcolepsy. That figure was for the one vaccine in one country which appears to be the only example in most people's living memory of a vaccine possibly causing long-term side effects (it's not even proven the vaccine was the cause). There have been tens of billions of vaccines given during this time period and this is the only example where there may have been long term side effects.
I've also mentioned the cutter polio vaccine and the 1976 swine flu vaccine which seems to have caused an uptick of GBS.
> There have been tens of billions of vaccines given during this time period and this is the only example where there may have been long term side effects.
No, there are other examples, the other two I just mentioned are from memory, I suspect if I go research I will find more (I don't have the time). You know what else is common to those other two cases? They were rushed (pandemrix wasn't AFAIK).
SARS-Cov-2 vaccines were all rushed, and the safety protocols used to confidently ascertain those billions of vaccines were NOT followed - The standard is to wait 2-4 years to see that there's no ADE or other issues.
I am pro-vaccination. I don't understand why it is hard to acknowledge and discuss the risk profile of vaccines - they re not risk free. Excuse me if I don't automatically think a rushed vaccine is perfectly safe.
> I've also mentioned the cutter polio vaccine and the 1976 swine flu vaccine which seems to have caused an uptick of GBS.
That Polio vaccine wasn't a side effect of the vaccine though, it was an issue with people accidently getting injected with a live virus. Since no live virus is even remotely involved in any COVID19 vaccines it has zero relevance here. Even if they were, we have 60+ years of history with no similar incidents since then.
> I suspect if I go research I will find more
You really won't. I've been reading about this extensively during this period and those are the only examples where there may have been long term effects that anyone can point to.
I qualified my original comment with "in most people's living memory" and didn't include the '76 swine flu vaccine because, frankly, I don't think pointing to an issue that happened 44 years ago in a field that has seen pretty significant technological advancement in knowledge, methods, and manufacturing processes really makes sense.
> why it is hard to acknowledge and discuss the risk profile of vaccines
My issue is not that there's isn't some theoretical risk, it's that it just isn't put in context of how minute it is. In all likelihood your risk of facing long term effects from a car accident happening on your way to get vaccinated are higher than anything that could happen from the vaccine. And both those risks are, of course, many orders of magnitude less than your chance of suffering long-term effects from catching COVID19.
> Since no live virus is even remotely involved in any COVID19 vaccines it has zero relevance here.
Your omnipotent knowledge is inspiring. We have absolutely zero years of experience with RNA based vaccines. We had incidents with vaccines, not of the same kind. Ergo, there's a non zero probability we will have incidents in the future, by any reasonable inference.
> I qualified my original comment with "in most people's living memory" and didn't include the '76 swine flu vaccine because, frankly, I don't think pointing to an issue that happened 44 years ago in a field that has seen pretty significant technological advancement in knowledge, methods, and manufacturing processes really makes sense.
That's really painting a target where your arrow landed. Most people's living memory does not include e.g. the 1918 pandemic or the bubonic plague, or atomic bombs, or thousands of other things we're proactively defending against and of which we have better understanding but are still an issue. If "living memory" is your criterion ... well, I wouldn't describe it as anything but completely arbitrary.
Within living memory you have totally understandable and preventable things like Fukushima, the nestle mother milk fiasco in Africa, and others. We had enough understanding to stop all of them, and yet they happened. Every single SARS-COV-2 vaccine manufacturer has gotten government immunity from future claims, which aligns their incentive differently compared to vaccines they have produced in the past. They have become too big/important to sue - much like e.g. the fukushima reactor operator. Given this distinctly different incentive structure, rushed schedule, novel RNA delivery system - your belief that the past is a good predictor of the future is unscientific (at the very least, unbayesian without a ton of nontrivial priors you don't bother stating).
> And both those risks are, of course, many orders of magnitude less than your chance of suffering long-term effects from catching COVID19.
Ah, about that. Do you have any actual data about that? Because the best summary of "long covid" evidence I found was written by an MD, is summarized here[0], and can further be summarized by the word "lacking". I spent a lot of time looking for actual data about long covid (not anecdotes), and this summary is better than what I was able to find myself (but I do urge you to read it - do introduce it to your "living memory").
I wonder if because the Oxford vaccine has taken an already tested and approved vaccine approach it has a higher chance of safety than the other 2 which use a new approach that has never been approved by regulators before.
FTA: "The Oxford vaccine (ChAdOx1 nCoV-19) is made from a virus, which is a weakened version of a common cold virus (adenovirus), that has been genetically changed so that it is impossible for it to grow in humans. Adenovirus vaccines have been researched and used extensively for decades"
I think the cold storage issues are a bit overblown.
Apparently the pfizer and Moderna vaccines will keep for 30 days at refrigerator temps after thawing out. You can ship in dry ice and then I can't imagine the vaccine sitting around in any doctors office or pharmacy for longer than 30 days.
Another huge differentiator is price. At $3 to $4, many countries will jump on board ASAP and stay away from the expensive vaccines from Pfizer and Moderna.
>At $3 to $4, many countries will jump on board ASAP and stay away from the expensive vaccines from Pfizer and Moderna.
The price difference will likely remain substantial, but in case anyone is unaware, the difference is currently greater due to AstraZeneca pledging to the sell the vaccine at cost "during the pandemic", while Pfizer and Moderna have indicated that they fully intend to profit. [1]
Once AstraZeneca deem the pandemic to be over, the price will likely rise.
It was reported a few months ago that internal AstraZeneca documents showed them projecting the "Pandemic Period" to end on 1 July 2021. [2]
To be fair, Johnson & Johnson (a US company) also made a similar pledge to AstraZeneca.
These two companies have collectively received more than $1.5 billion from the US government [1]. As I understand it, Pfizer have not taken any federal funding. They do have government purchase agreements, but they are dependent on Pfizer delivering a viable vaccine. Their partner BioNTech received German government funding:
Berlin gave the German company $445 million in an agreement in September to help accelerate the vaccine by building out manufacturing and development capacity in its home market. [2]
I don’t think the data bears this out exactly. US healthcare tends to optimize for access and quality to the detriment to cost. As the saying goes: access, quality, or cost... you only get to choose two.
The US tends to measure better than any comparable country of its size on those two metrics (and quite poorly on cost...but some of that is because the US funds about 50% of worldwide medical R&D)
The US healthcare is good only when considering those who can pay to access it. But since large swathes of the US population cannot afford to have access (expensive insurance costs, even with Obamacare support), this becomes a mute point. If that is the metric, then even Brazil (and many other 3rd word countries) also has good medical care, because it works for the small percent of the population with money to access it.
And in fact this is one of the big differentiators between 1st world and 3rd world countries: if the population has access to quality services, in health care or other important areas like education and sanitation. The US seems to be designing its systems to become a big 3rd world country.
> The US healthcare is good only when considering those who can pay to access it.
False: The third leading cause of death in the US is believed to be preventable medical errors. You can go to the best institutions in the US to get care, along with seeing the very best doctors, but you cannot evade a statistic like that, even if you are in the 1%. See: https://www.npr.org/sections/health-shots/2016/05/03/4766361...
The truth is that you can be in the top 1%, sitting on a mountain of cash, and still lose an unfathomable amount of money, even while insured, if you have cancer or a rare disease. Both of which are actually common.
It is not the doctors who are the problem here with respect to the medical errors: it’s the healthcare system. A good read on what’s wrong with the system is the short book Our Malady by Timothy Snyder.
If you want to stay alive long term, you may want to consult HealthData.org which analyzes each country’s healthcare systems in depth along with outcomes. The group is world renowned. Ironically, it is also the IMHE group that does the coronavirus statistics that everyone consults.
Personally, I am an American culturally, but I became an EU citizen (Croatia) over the US healthcare system. I never plan on working in the US. I do select the country I am working in now due to healthcare.
Your points are baked into the data that I linked. The metric within is "HAQ Index" which stands for "Healthcare Access and Quality". I.e., access is part of the measure. In the US everybody has access, which is part of the problem that drives costs higher.
E.g., if you don't have insurance you can walk into an emergency room and get treated even if it's not an emergent situation. If you don't have insurance, there is a higher risk you won't pay. That cost then gets spread to others who do.
You probably don't know how the US system works. The only access that is guaranteed by law is to emergency services. If you don't have a paid insurance (through your employer or yourself), then you cannot access preventive care or otherwise normal medical consultation. Millions of people in the US don't have access.
For example, if someone needs to treat cancer, it doesn't make any good to go to an emergency unit: they will discharge the patient as it is not an emergency situation.
>if someone needs to treat cancer, it doesn't make any good to go to an emergency unit
That's because the ER is meant to stabilize a patient, not cure chronic disease. Which is to my point: people will forgo preventative medicine until their condition deteriorates and they need to be stabilized in an ER. People get their non-emergent conditions treated all the time in American emergency rooms.
E.g., if I have diabetes, an ER will not put me on a long-term treatment plan. But if I ignore my disease until I start having hypoglycemic symptoms an ER will treat me until I am stabilized enough to be released. Is this the best system? Absolutely not, but it's much different than saying "only the rich have access to healthcare".
FWIW, I used to work in healthcare, including redesigning ER processes
And how would anyone know if he has diabetes (for example) if the person doesn't have regular visits to medical facilities? In such a case they will go to emergency only when an emergency happens, probably when it is already too late. By saying that such a person has access to health care, you're just redefining health care to "emergency health care".
If this was not enough, hospitals are catching up to the "loopholes" in the law and abandoning poor neighborhoods, to make it even harder for people to use emergency rooms.
In the example of diabetes, many people are diagnosed when they show later term symptoms that require an ER visit. Since it's chronic, they won't be "cured" of the disease, meaning an ER can be their main mode of healthcare and the main mode of being diagnosed.
You may not understand the nuances of the article you referenced. Take Detroit, one of the cities used to support the claim in the article. The baseline decade used is the 1960s. Detroit has only about a third of the population it had in the 1960s so it's not rational to think they would maintain their previous healthcare infrastructure. Further, much of that population left for the suburbs of metro Detroit, meaning the healthcare facilities being built are just following the population demographics. Add onto that the point that healthcare has changed dramatically over the last 60 years with much more emphasis on outpatient care, and there are rational, non malevolent reasons to decrease the number of urban hospitals
Curious, in your healthcare experience, what would you estimate is the percentage of people who do have good insurance, but don't get preventative care by choice?
E.g. for myself, I have good insurance, but I don't have a "primary care doctor." I don't go to the doctor unless I'm injured or sick. And I don't mean a sniffle or cough, I mean sick as in I have felt awful for several days.
I don't think I have a good representative sample because facilities I worked for were a specific sub-population that would probably have a very high percentage that fall into the category of "no need for healthcare until something is broken or bleeding profusely"
With that said, it seems to be quite a bit and skewing higher for males than females.
If you have insurance and are not going for a routine exam once a year, you're doing a disservice to yourself because you miss the opportunity to catch issues that can be easily fixed when caught early but catastrophic if not. In fact many corporate policies require people to have regular exams exactly for this reason.
A lot of countries do not do “yearly physicals” like the American healthcare system recommends. This is because in countries with universal healthcare, patients within the country go to their GP/Primary Care Doctor far many more times on average than the typical American. So, in many countries, this practice is non-existent, basically because people just go to the doctor whenever they feel it is necessary—and far more often than the typical American does.
The average American sees a doctor 3 times per year. In France it is 6-7 times per year. In Japan, it’s 13 times per year. This statistic is directly linked to the cost of care.
In Europe, Canada, Australia, etc everyone has access. Why doesn’t access drive up their cost? Clearly access isn’t what is driving up the costs in the USA.
Because it's not as simple a model as "access vs. cost". It's access vs. quality vs. cost.
Canada's HAQ index in 2015 was 87.6 vs. 81.3 for the US. However, Canada spent about $27B US on R&D vs. $495B for the US. On a per capita basis, the US outspends most the world on medical R&D. That drives the US total healthcare costs up while helping to drive down the healthcare quality costs elsewhere. To a certain extent, the US subsidizes the healthcare costs through much of the world, effectively allowing them to optimize for a 2 parameter model while the U.S. must still deal with a 3 parameter model.
Yes, the US spends much more per-capita on medical R&D than other countries. But how do we know all this money is going into real R&D? How do we know most of it is not going into e.g. me-too drugs?
That's a potential real problem, but the concern should be across the board (i.e., how do we know other countries aren't funding me-too drugs) so it doesn't really help illuminate any disparity between countries (which is the context of this discussion).
I'm not trying to be dismissive, I just don't know how it's germane to the discussion unless we view all the other data through the same lens. The data I linked is per country in absolute and per capita basis that tries to put it in unbiased terms.
Are you claiming the US is disproportionately funding non-useful research? If so, how do we measure "useful" research funding?
I do not know how to objectively measure useful research funding. However, this discussion reminded me of a graph I saw on the wtfhappenedin1971.com site [1]. It's not direct measurement of R&D development, but it sure as hell doesn't paint a good picture for all the spending that's going on. I wouldn't be surprised if a similar allocation of funds was happening in medical R&D as well.
Yes, I'm familiar with that graph. There's a similar one for college tuition in the U.S.; interesting that both are industries where costs have been growing at more than GDP year over year.
However, the point between comparing countries still holds. If you use older data, you'll see that the U.S. had even more disproportionate R&D funding
The important issue is that R&D spending is not a good measure of outcomes. A lot of R&D spending goes to high administrative salaries, equipment, facilities (real estate), and related costs that do not translate into outcomes.
What would you propose as a better metric of innovation?
I don't think there's a single perfect measure but if you put it in broader context of measures like Nobel prizes R&D spending, patents, etc. it does seem to paint the picture that the US disproportionately contributes to medical innovation.
It's very similar to the measure of health. There is no single great metric. Using a single metric like BMI or blood pressure is flawed. However, you can get a clearer picture if you bring together multiple metrics.
this is completely missing the point, people don't take chronic or slow-developing issues to the ER so they get worse and have catastrophic consequences resulting in both worse health outcomes and more expense because by the time they do come to ER it's a more serious intervention = $$$$
I addressed that in a different comment (I think we submitted comments at roughly the same time).
I completely agree that preventative healthcare is lacking, partly due to the system and partly due to culture. If the OP had originally said "preventative healthcare" I wouldn't have much to disagree on, but they used a blanket statement implying only the wealthy have access to healthcare in general.
The US also gives free preventative healthcare to many subsets of the population
As someone who migrated to Germany from Turkey, people like me (and everything we are involved in) are "German" when we do something they're[0] not proud of, we are "Turkish" if we ever come close to success, and "of Turkish descent" in the normal times. Of course it depends who you are asking :) It's a bit annoying to be honest but not a huge deal.
I didn't mean to make any judgment about the "Turkishness" or "Germanness" of Drs. Şahin and Türeci. I just mean to clarify that BioNTech was founded and is based in Germany, just as Google is an American company (not Russian-American) even though Sergey Brin was born in Moscow.
I have read it‘s a bigger problem and a source for islamism, especially for the 2nd or 3rd generation of descendents of immigrants: When Germans still see you as Turkish, but Turks see you as German, it makes sense to a) be angry and b) search for some other identity.
> The AstraZeneca vaccine also has 90 percent efficacy when used twice
No it doesn't. Both dosings use two shots, and the "90%" number from the smaller dosing is from an unreliably small sample set of 33 infections -- it could easily be 70-80% by next month when more data comes in.
I don't think we know based on public information. Some media report "up to 90%" which suggests the upper bound of the confidence interval, rather than the centre. Could also be a very wide CI, that overlaps with the standard dosage.
That's a fairer statement than the original which seemed biased towards only reporting the lower end of the interval without acknowledging the upper bound.
At the moment possibly wider error bars don’t come from just “33 infections” but more from possibly smaller number of those who received the observed treatment.
The bars are to be calculated using conditional probabilities.
>These two companies have collectively received more than $1.5 billion from the US government [1]. As I understand it, Pfizer have not taken any federal funding. They do have government purchase agreements, but they
So where did Pfizer's capital come from to shoulder these costs? It didn't come out of thin air, they've accumulated capital from somewhere. If not from taxpayers, someone is subsidizing Pfizer's expenses through Pfizer's revenue stream. Taxpayer subsidies really make sense here seeing how this issue effects everyone.
> someone is subsidizing Pfizer's expenses through Pfizer's revenue stream
Companies taking a portion of what they earn from their existing products and investing this money to create new products is beneficial, and we should have more of it.
Additionally, while this is probably not the case for Pfizer, another possibility is that a company can take outside investment to fund development of a new product.
Not the OP, but what she/he is probably hinting at is that the majority of Western Governments (i.e. both the US and the EU) have poured trillions of dollars/euros into the market as the pandemic started, money that has helped the capital markets stay afloat (and even more than that).
Without those trillions of dollars/euros most probably the capital markets would have been down by at least 50% (my guesstimate, or at least that's where we were headed mid-March), which means that the money available to companies like Pfizer would have been a lot less.
As such, Pfizer saying that they didn't receive federal money is technically correct, but without federal money most probably their market value would have been a lot less right now.
A 40-50% reduction in share price would have most probably eliminated the dividends completely, especially in a very adverse deflationary market, which most definitely would have seen the most of that $10 billion sum allocated to other things than R&D.
Pfizer's cash situation or ability to spend/pay a dividend has nothing to do with stock price. Pfizer does not have their cash balance invested in other stocks. Ability/willingness to pay a dividend has to do with excess cash.
To the extent there's any relation, it's a high stock price that discourages paying a dividend. If the dividend yield will be basically nothing, why bother spending down precious cash that could be reinvested (because obviously the market values future cash flows a lot more than current ones).
Deflation might encourage a little bit of holding of corporate cash rather than spending it on R&D, sure. But even then I think you're overstating the case.
The question was simply to stimulate a more holistic view of the example at hand: that Pfizer did this on their own and essentially didn't need/get any financial help. Sure, Pfizer didn't receive direct subsidy in the short term related to COVID R&D and is taking on risk.
But let's look at this more holistically. Pfizer and pharma benefit a reasonable amount from public research. Pfizer has received their fair share of governmental funding in the form of products, services, and research:
https://www.usaspending.gov/search/85a918fa6adf5152dbac723d2...
They've also been subsidized by people with illness over the years that isn't related to COVID (directly or through their insurance provider pools). It's in other cases the previously sick that have padded Pfizer's profit margins enough to enable them to accumulate enough capital they could take on this sort of risky R&D. Theres also the costs of enabling laws and defending their IP rights from external pressures the US pushes.
It may not be direct subsidy but there are plenty of indirect subsidies that enabled Pfizer to do this. Let's stop pretending these businesses pull themselves up by their bootstraps to success and take on all the risk: they don't. They very often take low risk returns and transfer to high risk and use subsidized activity (e.g. federally funded research) to their advantage. Anything high risk like pharma is prone to failure and needs assistance.
Should we continue assistance? Absolutely, I think so, it's good for everyone. As one parent mentioned, it is good to see these businesses reinvest in further R&D that lead to new discoveries in therapy and treatment as opposed to simply hoarding capital.
Apparently the thought of the narratives that Pfizer didn't pull themselves up by their bootstraps financially makes some people cranky. Everyone needs assistance (especially in high risk arenas), let's not pretend that assistance doesn't exist simply because its indirect, time delayed, and being shifted around.
I agree with your overall point that it needs to be looked at holistically, but I don't think I agree with your stance on some of the subsidy arguments.
A subsidy is, by definition, a governmental funding mechanism. "People with illness" who used Pfizer products in the past aren't subsidizing the COVID vaccine anymore than I subsidize an automobile manufacturer making pickups when I buy my tiny hatchback. It's built into the business model and not really a "subsidy".
I agree with you in terms that we shouldn't view these companies as operating in a vacuum, I just don't think the idea of the markets being propped up is the most congruent way of framing the discussion. Pfizer benefited along with most other publicly traded companies, irrespective of their COVID vaccine.
Is there somewhere any numbers on how much exactly does it cost? What portion is really "research" and what portion is marketing budget? How much trial phase 1/2/3 cost etc?
When I studied pharmaceutical sciences ten years ago, the rule-of-thumb was that it cost around 1 billion dollars from idea to the product being launched. That's only r&d costs and regulations have become stricter over the years, so I imagine the cost has risen since then
I’ve seen this number with some justification being the amortized cost of a successful product, which covers r&d and marketing but also the failed attempts that lead nowhere in between.
There are plenty of 50-100M pharma startups; they wouldn’t exist if your number was right.
>There are plenty of 50-100M pharma startups; they wouldn’t exist if your number was right.
Isn't there a selection bias in that the startups that got to 50-100M survived because they were lucky with a candidate treatment. The ones that failed were the ones that never found a candidate in time? The difference being that large pharmaceutical companies have to swallow ALL the failures, whereas startups can "just" die.
Not to say that pharma companies don't have some fat that can be trimmed...
>which covers r&d and marketing but also the failed attempts that lead nowhere in between.
How do you account for the failed attempts?
As yomly alludes to, pharma startups exist because they don't own the risk - their investors bought it when they were funded. Big pharma does own the risk.
You sum the expenditure and divide by number of successes, with some accounting for the delay. It is actually much easier than trying to figure out the cost of a specific drug, because research is sometimes shared.
"Pharma start-up" is a broad definition which might not only be drug development and there might already be work done on their product before they look for funding
A company that is spun out from a PhD project in a research group, that has done a lot of the groundwork on grants will need less funding
Same goes for a start-up that for instance make non-invasive assays for diagnosis, since the documentation requirements are lower for such products
Producing something that has to be injected into humans is an entirely different league, since the amount of documentation required for such products is staggering
The cost for marketing will vary significantly depending on your definition of the word, and I suspect that it might be misconstrued as only being "commercials and paid holidays for doctors"
GP said idea to product costs 1B just for r&d. That and 1B amortized over failures (and including marketing) cannot be true at the same time unless there are no failed attempts and unless marketing cost is zero.
I've seen you mention marketing several times. What expenditures would you include as a marketing expense?
I'm also not sure what you would define as a failure. Drug development often starts with several candidates for a target. Over the cause of development the list is trimmed, as candidates show lack of affinity for the target or have side-effects that make them unviable. Would you consider each of the excluded candidates a failure?
> I've seen you mention marketing several times. What expenditures would you include as a marketing expense?
I don't get to define that, companies do, but basically it includes everything that does not involve a lab, technician, doctor, nurse, statistician/programmer, etc. The US and the rest of the world are quite different here - if you've ever watched US broadcast in the evening, you'd see TONS of ads for prescription only medicine ("suffering from foo? Ask your doctor about bar"); that's marketing. Taking three hundred cardiologists on an all-expenses-paid 7-day cruise with one 30-minute "purely informative lecture about our new drug" and 7 days of fun? That's marketing too. Lobbying to congress? That's also marketing.
Outside of the US, the marketing budgets are smaller and less overt - but the cruise-style legal bribe-like events are prevalent everywhere.
> Would you consider each of the excluded candidates a failure?
Possibly. You've described one style, but it's not the only one. Many times, it's a weird result from some other research (how Viagra was discovered, how DCA tests were started).
But many things are essentially complete and utter failures - you have a line of research where no viable compound was found at all. BiondVax just failed a 15-year mission trying to develop a universal flu vaccine. Remdesivir is essentially failed even though it is FDA approved (It failed for Ebola; if you look at the data critically, it failed for SARS-COV-2 -- which the WHO's recent studies show even more clearly).
There is some benefit from this research - new techniques, often new devices - but the drug itself is a failure in the sense that it will not generate any income to the company.
Edit: just saw your earlier comment about marketing. It is those things (which you and I mentioned) and a lot more, but it is basically for the company to define in their books and a rule of the thumb would be “an expense a university department developing this to completion without expectation of profit would not have to spend”
The usual course for a biotech is multiple raises as the drug progresses through trials and an early IPO. At each step investors see it as a surer shot.
It's not so much the cost, it's also the delay. At a 5% cost of capital, and a 10 year lag between R&D and final approval, your real cash flows are 40% lower due to the delay. At a 10% cost of capital, they are 60% lower. Sales also take several additional years to ramp up.
This doesn't apply so much to Covid vaccines, as the time frame is accelerated and demand is already high.
The 1bn is only the out-of-pocket cost for development and doesn't factor in for instance opportunity cost. If we include everything required to develop a vaccine, I'd imagine we're looking at something north of 2.5bn
There's so many ways to calculate the cost, that I think it's more important to be aware of the assumptions made for the estimate, than the number itself (which I also failed to do in my original answer)
I think people underestimate the cost of drug development, because the numbers are so big, that it doesn't seem realistic for companies to survive
I talked to a bunch of CROs about the cost of Phase 3 trials. It varies, but is roughly $10,000 to $15,000 per patient year.
Pfizer’s trial will run for 2 years, so ~$900M for the trial alone. That’s excluding all the work to scale up the production, regulatory filing, distribution, etc.
Is it really $10-15k each additional patient year requires or it's more of "total cost was this much, we divide it by number of patients". Where do this money go to? Fx, with these covid trials, 40000 people in pfizer trial, half a year cost would be $200-300 mln. People presumably weren't paid for this. Of course there's some work by doctors that needs to be paid for, but that can't be this large amount. Also, does this all assume USA standards of pricing? Because in rest of the world healthcare is much cheaper.
I just think big pharma are fundamentally ok with huge cost for trials and are not motivated to decrease it/make it more efficient, since they're ok with their pie being larger. They will just shift costs to healthcare system and will be happy with larger profit.
Ha! You think big pharma likes spending that kind of money on trials? I’ve been a part of those negotiations with the FDA. It costs that much because the company says “we believe a 6 month trial is sufficient to prove both safety and efficacy” and the FDA says “if you want it approved, you need to collect 2 years of data”.
Now, $10-15k per patient-year is for a typical therapeutic. And that is an average across global trial sites, not just the US. It’s not much money. You go a 15 min doctors appointment and your insurance is billed $150. Now imagine going 1 per week and having multiple tests run each time. Or having to stay in the hospital for a day when the drug is administered. You can burn through $1,000 per month pretty damn quickly.
I don't see a reason they would be really against it. FDA says it to everyone, so all companies in same condition. And they can shift cost to healthcare system and have larger revenue. They probably don't mind their pie as a whole being larger, because having revenue of 50 billions and profit of 10 billions is better than revenue of 5 and profit of 1, even though proportionally it's the same. All big pharma companies are massively profitable, fx Novartis net income in 2017 $17.8bln on $50.4bln revenue. Pfizer's $14bln operating income on $53.6bln revenue in 2018. And it's year after year. They really don't seem to suffer from those high costs trials. Also, Pfizer reports only $8bln on R&D in same 2018. I'm sure there' a lot of inefficiencies in those trials, same as it turned out vaccine could be created in year instead of a decade. (btw, previous large scale epidemic of swine flu was largely profitable for pharma companies). They just don't have incentive to reduce the inefficiencies.
You're telling it's not just US but then you cite high healthcare costs (retail vs large scale trial, definitely can be cheaper at scale), which is much cheaper outside of US. I would be very interested in reading numbers of detailed case study of creation of some real world vaccine/drug.
They probably don't mind their pie as a whole being larger, because having revenue of 50 billions and profit of 10 billions is better than revenue of 5 and profit of 1, even though proportionally it's the same
It doesn't work this way. Pricing of pharmaceuticals is independent of the cost of development. Nobody will pay $200 per Covid vaccine dose just because the cost to develop it went up 10x. Every extra dollar spent on development, is one less dollar of profit.
That's why some drugs never make it to market - the cost to bring them to market and the low price means they'll never be profitable.
Even if it doesn't happen for each and every drug, that can easily be the trend on average. And it probably already happened with covid vaccines. Moderna comes out and says it will cost ~$30 per shot. Why not 3? And for others drugs, when price goes into thousands and don't have much competition that easily can be the case.
I'm a volunteer for this vaccine, in the first month I have three in-patients visits, involving two inoculations, 6 blood draws, 2 Covid tests, and three nasal absorption tests. My first visit lasted a little over three hours including a very comprehensive medical history and physical exam, and time taken to ensure that I was giving truely informed consent. I interacted with three medical professionals on the first visit, sometimes in the exam room, and sometimes via phone from the exam room to protect each other from long in person indoor exposure. Like any medical visit this year, a considerable amount of PPE was used. I was given an app use daily to record my health, and a digital thermometer so that all subjects are using the same calibrated equipment. Having reported a headache two days in a row in the app, there was a remote phone call follow up by a research clinician, in addition to the planned check in phone calls that I haven't mentioned. They do pay me a very modest ammount, so I've bought myself a couple of ebooks after paying for big city parking near the research clinic. They need to pay for that office space. Before I entered the study I needed to interact with recruiters, to qualify that it was safe enough for me to participate and to ensure that they were getting people from a variety of backgrounds. They needed to be ready to respond if I had a severe adverse reaction to the the trial vaccine. There is an entirely separate independent review board that I can go to with questions. In the event that I had Covid symptoms, there is an entirely separate set of assessments, visits and samples taken.
Given the amount of work being done by this and other research labs hired Astrazeneca, and comparing this to quotes I've received for a very modest UX usability studies, it's hard to see see this an sort of money grab.
No, it's not. Private R&D spending is at least doouble that of the gov't. Look up the budget of the NIH and compare it with the R&D budget of big pharma.
BioNTech developed the vaccine now mass-produced by Pfizer. For that, they received $445m from the German government. So, as a tax-paying German citizen I can say, not only will I do that, but even better, I already did.
It also feels deeply wrong to pull the "but all the research efforts that did not lead anywhere" argument, when Pfizer did not do the research in the first place. They should get compensation for organizing the huge trial, of course; that expertise was why they were on-boarded in the first place. And nobody expects them to manufacture that stuff at loss or cost. But we should not accept public money buying them goose laying golden eggs either.
Nobody’s getting a goose laying golden eggs from a covid vaccine. It’s a one time, relatively low-cost vaccine that is going to go out of demand once the population is immunized.
Oh, and now there are multiple competitors in the market.
Only if the vaccine gives permanent immunity, which I haven't found any research suggesting that it will. In all likelihood, it will be necessary to give yearly booster shots, so the companies developing the vaccines will be able to sell vaccines every year
The quantity of vaccines needed will make even a $0.50 markup worth billions of dollars every year
You can't measure long-term immunity on a virus that's only been in the wild for ~11 months. That said, all the recent studies I've seen show no signs that immunity is going to drop significantly after a year.
I hate to link to a Youtube video, but this doctor walking through the research in the first part of the video is honestly better than any news article I've seen:
https://www.youtube.com/watch?v=gFeJ2BqCFY0
Thank you for the link. The study definitely suggest a best-case scenario is viable. I do however think that the sample population of 183 subjects is too small to support the conclusion in the paper. The study only got a single sample from the majority of the participants andI couldn't find any indication of how many subjects from each location participated (or which locations were included outside of California), which makes me think it might not be a representative population used
I also noted that 40 of the participants were excluded because they had no PCR test done to confirm covid and no antibodies were found in the assay. This is in my opinion a major flaw, as the subjects could have been infected, but had no antibodies left, when the blood sample was taken
Finally seven of the 18 authors declare competing interests, which might have affected the research
Getting back to your post itself, I agree that you can't measure immunity for a longer period than the virus has been around, but that also means you can't say that there will only be a need for one round of vaccines, which was what I was disagreeing with
It might very well turn out, that you gain permanent immunity for a specific strain off the virus, but unfortunately that immunity also introduces selective pressure. Whether the virus is able to mutate in a way that bypass existing antibodies in a subject is obviously still an unknown, but we have seen that it's able to jump to other species like mink, which caused the emergence of the Cluster-5 variant
Since the virus is able to use other species as a reservoir and selective pressure is being introduced, I think it's reasonable to prepare for a scenario, where a vaccine won't be a permanent fix
Vaccines are not a great business in general. (Which is not the same as saying they're unprofitable.) But one reason vaccine makers are generally indemnified against lawsuits in the US, it that at least some companies would probably pull out of making vaccines if they weren't.
These nickle and dime arguments are for "old normal".
The society at large is making huge sacrifices and making painful changes to address this collective problem. Are these companies part of "Human society" or not? If they are party of Humanity, then they can make 'adjustments' as much as we are asked to make adjustments.
Have these companies provide a detailed list of expenses for researching and developing this vaccine, review that, pay it as a one time cost and THEN vacate the patent.
They then get to recover their R&D expenses and make a smaller but probably decent profit from its production.
Bankrupt? Not many. Bought for pennies on the dollar? Plenty. Where is Upjohn? Parke-Davis? Schering-Plough? All companies with multi-billion dollar sales figures and all swallowed up when the money stopped coming in.
And if you fold in the start-ups who have one shot and if it doesn’t work out? Plenty of those. They go bankrupt.
Busting the patents on Covid vaccines would be “socializing the gains and privatizing the losses”.
There are currently 54 vaccines being tested on humans. Getting the necessary data to obtain approval for human testing requires a lot of funding. Testing on humans requires a lot of funding. In the end, maybe 4 vaccines will be used. Do you think the companies that produced and tested the ~50 vaccines that will not be used will get their investment back?
This isn't responding to the OP's point, which was that war profiteering (making money by providing weapons to kill people) is morally different from selling vaccines (making money by providing medicines to save people's lives).
I'm very familiar with the perverse outcomes that emanate from profit-driven medical research, having been personally affected by illnesses that the mainstream medical science community sees no incentive to invest in.
But the reasons and ethics of the system being the way it is are separate from the reality of what it is for the purposes of getting things done in the here and now.
For better or worse, as things stand right now, pharmaceutical companies, like other companies, need to make profits - or at the very least avoid crippling losses - in order to survive and continue doing their work.
That includes covering the formidable costs of the many research studies that go nowhere and yield no revenues.
I'm sure you wouldn't find a single person in a pharmaceutical company who would feel good about withholding treatment from any person with a life threatening illness. But what they also have to care about is remaining in business so they can treat and cure many more people with serious illnesses.
Regarding vaccines and altruism I suggest you read up on Jonas Salk, who developed one of the first successful polio vaccines[1]
Money quote from linked article:
"News of the vaccine's success was first made public on April 12, 1955.[7] Salk was immediately hailed as a "miracle worker", and chose to not patent the vaccine or seek any profit from it in order to maximize its global distribution."
I do not dispute that altruistic people exist, and often do great things.
But I also know that my grandmother suffered terribly from rheumatoid arthritis, and it destroyed her life. Long after she died, enbrel was developed for profit which was the first really successful treatment for it.
No profits => no treatment => misery.
You can sit around waiting for and hoping for someone to step up and sacrifice their time and money for your benefit, but I prefer the much more reliable method of paying them.
Not to take anything away from his contribution, but it's a bit more complicated with Salk.
The organizations who funded the research looked into the viability of a patent and concluded it wouldn't have succeeded.
"the idea of patenting the vaccine had been directly analyzed and the decision was made not to apply for a patent mainly because it would not result in one."[1]
The distinction should also be made that a patent doesn't necessarily affect global distribution. It just gives the rights to license the technology. They could have patented it and then licensed it for free.
Here comes my old publicly traded corporation rant: a company with a well defined owner, even with a well defined group of owners, would, given the opportunity, profit handsomely. But not overdo it. They'd rather be seen as a global saviour, not as a global ransomer.
Enter public trading: the opportunity alone for global ransoming will inevitably become the projection that defines the street price for shares and once valuation is up there ransom-level profits would suddenly appear not excessive but appropriate, given the level of paper investments of the latest, valuation-defining round of buyers.
Private (as in: not publicly traded) is indeed pretty much equivalent to publicly traded if it's a private ownership structure consisting of VC funds. But that's a startup bubble peculiarity, elsewhere private ownership either means being a subsidiary where the parent ownership structure transitively applies (strictly speaking, the VC funded startup falls into this category as well) or a much more conventional setup where the role of outside investors is taken by old-fashioned banks whose possible returns are strictly limited to what the credit contract says.
The main issue is identifying what anti-social behavior is. It's easy to say "coal is anti-social! don't you care about the environment!", but it's just as anti-social to just shut down an industry and say "best of luck, I heard you can move to California and build websites in JavaScript". Often times there just aren't easy answers.
I also want to push back on "everything commercially successful is run by tyrants" kind of narrative. I get the frustration, but these blanket, ideological statements do not help anyone, anywhere. Do you make money? I guess you're a tyrant!
Let's not forget, the countries that we put up on a pedestal as the shining examples of how a country should be run (Norway or whatever) are very much capitalistic countries with free markets, IPOs, and commercial companies. I hardly see businesses there characterized as tyrannical.
I do really get the frustration, but it needs to be directed at the failures of our elected representatives. Not, commercial entities.
> The tyrannical boss is a classic trope due to the necessities of competition.
Eh, I think that’s kind of old-school thinking.
> Companies are unlikely to stay profitable if they’re overly generous. They need to profit handsomely to survive.
Yep. That’s fine. (Also ignores low-margin industries that rely on volume, but whatever).
If you want a modern society, people have to be able to take risks with their money in order to make more money. Otherwise we can go back to subsistence farming. Do you work? You’re charging a profit. How evil of you! Being a few steps removed from the transaction doesn’t make you any less guilty of profiteering. You’re just as bad as these tyrannical CEOs, the difference is you’re a sucker for building their product while they make money hand over fist.
(I don’t actually believe the last part, but w/e).
Today. Just 1 year ago the next pandemic was vaporware. In hindsight we know that covid happened, but there was no more reason to think it would have than any other unlikely event.
I doubt if vaccine research can be done just by a group of interested people. It's not a paper-and-pencil affair like pure maths. You need a lot of computers, drug manufacturing machinery; then you have to run big, well-organized RCTs. If you've got an example of volunteer-driven health research at scale, I'd like to hear about it.
Biontech didnt do vaccine. They pivoted because they saw a big opportunity using their approach might lead to a vaccine for Covid. So to justifies this pivot (and get the investments into the company) there need to be a possibility of big profit at the horizon.
A profit opportunity requiring significant investment has led to fast and fantastic results that will benefit us all. But you want to punish the opportunists who've absorbed significant risk to bring us those results because you've decided their motivation isn't sufficiently pure.
I pray anyone of like mind is never in a position to enact such progress-killing madness and fear terribly that government is already full of them.
And besides, it is mind-numbingly complicated to calculate "at-cost" because as others have pointed out, that includes all of the dead-end R&D, ongoing legal exposure, interest on the loans used to cashflow operations at pharmaceutical giants, appropriate licensing of existing intellectual property that these vaccines are built on, and the million other ways money is spent to develop pharmaceuticals.
While I think the current system helps, let's not pretend that profit is the sole reason people decide to work in medicine or research.
We all have things (and people) in our lives who are probably a net negative in terms of financial outcome, but we enjoy them anyways because our value systems are more complex than just "maximize profit"
I agree that in cases of overwhelming national interests patents and licensing should be ignored if they stand in the way.
But: this is not a medicine made of a molecule that can be synthesised by the chemical industry.
Such a vaccine requires input from the creator and then specialist equipment to manufacture. Poor countries don't have the infrastructure to manufacture and the creator labs are not going to tell you how to produce the vaccine just because you ask them.
In any case, governments should pressure labs to enforce an low prove.
In the context of the vaccination rush I often wonder how military aircraft procurement was doing it when extreme r&d progress and extreme mass production were coinciding during ww2. New types were developed by companies (even the Soviets maintained a healthy competition between design bureaus) but once a type was established and in volume demand it apparently was manufactured wherever a production line could be adapted. Was that just free market subcontracting in the US or did DoD design bids come with something like a premeditated licensing option baked in from the beginning?
I think that the "free market" stopped to operate during that time. The whole economy was redirected to the war effort and everyone with it.
These programs were federally-funded with the goal to produce as much as possible. For production I'm sure that factories were financially compensated for the work.
I’m sure you’d be willing to play that game? Let’s say your job becomes “essential”. The company pays your costs (rent, food) and nothing more. I mean, to “profit” is unacceptable.
While off-putting, these same capitalist forces are what made companies like Pfizer possible in the first place. Where are the socialist factories? I do not see any communist, religious and/or otherwise motivated groups of people producing anything of value right now. Lots of noise, very little substance.
No, the main driver for the price difference is that this is a "traditional" vaccine produced using existing technology, while Pfizer/Moderna are newfangled mRNA ones.
Also, all 3 have made various noises about not making a profit etc, it's quite hard to sort out the marketing from what will actually happen at this point. Oxford/Astra have committed to supplying at least 100M doses to low-income countries for under $3 though.
As I understand it, whatever gets us to herd immunity more quickly is the best solution. That probably means a mix of both heavily tilted to the Oxford one.
This vaccine is cheap, 90% efficient and easy to get people vaccinated. The other ones are expensive, 95% efficient and difficult to get people vaccinated.
No, it means deploy everything we have as fast as we can. If we have a choice prefer the mRNA vaccines as they seem to be more effective. If you are in a city with cold storage abilities (most have this already, though how much...) the Pfizer is better, but only to reserve the Moderna vaccine for those who don't live so close to cold storage.
The Oxford is best only if you either live in a very remote place, or are a very poor place. If you rely on the oxford vaccine it will be a little longer to get herd immunity, but overall your costs will be cheaper.
But I must reemphasize, the above is only about logistics. Because most people live in cities, all vaccines will be distributed in big cities just to get the numbers they need. What ever vaccine you are offered first is the one to take. You personally are unlikely to be offered a choice other than take it or leave it.
If they actually get to 90% or more, why would anyone bother with the more expensive and cumbersome vaccines? Except that the EU already signed a deal to buy the vaccines from AstraZeneca, Sanofi and Johnson & Johnson.
Especially in the next few months, supply of all of these will be limited by production capacity and supply chains. Having multiple available means more doses can be delivered sooner.
Because there is only so much to go around in the initial stages, so they will buy whichever one is available to them. The 10x increase in price is peanuts compared to the ecconomic benefits of getting more people vaccinated sooner.
Additionally, lots of countries have already preordered all the major candidates, so in those cases its already spent money.
Because 95% efficacy is twice as good as 90%. And some people are willing to pay the $30 it costs to be 5% likelihood to have a non-functioning vaccine vs. a 10% likelihood the vaccine you just got won't work on you.
Aren't people worried about the fact that mRNA vaccines haven't been deployed before? I don't see much apprehension about that generally, but a few months of testing of a brand new delivery technique don't sound that extensive to me.
The delivery technique relies on LNP (lipid nano particles) which is fairly refined and existing therapeutics use today. There are potential patent violations though (both Phizer and Moderna possibly violating Arbutus patent) but it’s unclear to me how this affects distribution.
No judge in their right mind will grant an injunction when doing so will cost the lives of third parties. All the harms can be solved with a big check.
Yeah I'm not 100% familiar with the potential case here but I'd imagine it's in everyone's best interest to ensure that the medicine is not hindered in its ability to be manufactured and delivered and that the company that holds patents on the delivery vehicle (LNP) would be compensated justly.
It isn't a new thing for what it's worth. Going back to earlier this year it has been looked at, but we don't really have a clear picture on what will shake out.
We don't have evidence that is possible. There have been vaccines in the past that protected without stopping spread. We think that the reasons that happened don't apply, but we don't know that.
Sure, maybe I just don't understand this whole charity thing. When governments can print trillions of dollars to ,,help the people in the pandemic'', why a few tens of billions of dollars matter when real companies with real experts are doing real work all day and night without sleeping. Instead of buying back bonds, governments should pay companies that help in this situation.
Honestly, why would any 1st world country "vaccinate everyone immediately"? Wouldn't it be more prudent for a rich country to wait until 3rd world countries vaccinate first in order to see what the side effects actually are? Not to mention the fact that we know nothing about potential long-term side-effects.
The mRNA vaccines are better and protect more people. AZ leaves 10% unprotected, mRNA leaves 5%. That's a big difference if trying to get to herd immunity.
While for now just speculation and without a doubt Machiavellian, it could be that this price difference ends up a significant factor for major economies in their choice for an expensive vaccine. I guess we will know, if/when/once examples of individual discrimination based on what vaccine people received start emerging (hopefully, never).
Regretfully, it would be not the first example of major economies using the current reality as an excuse/cover to conveniently push political policies/agendas that would otherwise have been impossible to implement (at least not without violating laws/treaties and maybe even basic human rights). I have no intention to fear monger, but I believe way too many are too naive about some of the things that are currently happening. That is, mostly people within those major economies, for people in less fortunate countries already learned the hard way how double-faced those major economies turned out.
How all this will eventually turn out ... anyone's guess is as good as mine. I guess we will all learn, when the immediate emergency of the current situation is over. I would prefer to be/remain optimistic, but thus far there appear to be more reasons for caution and skepticism (at best).
I've read this 3 times and can't figure out what you're trying to say.
Are you saying that rich countries are going to intentionally choose more expensive vaccines, with the intention of suppressing the lower classes?
That's so rediculous. In rich countries (other than the usa) the gov pays for these things not the citizens. Even then, the expensive vaccine is only $40, that's within the means of most poor people.
Not to mention that would screw over the rich people who want to benefit from (vaccine induced) heard immunity.
> .. the gov pays for these things not the citizens ..
You do know that the only money governments have, is the money they got from its citizens, right? That is, aside from what they may have earned (though plundered or extorted might be more fitting) from other nations.
> .. the expensive vaccine is only $40, that's within the means of most poor people ..
You may want to reevaluate your knowledge about the rest of the world. That is, outside the USA and some the more affluent parts of Europe. Also, that vaccine probably won't cost "just" $40 equally for everyone.
However, believe whatever you want. Time will no doubt teach us all a lessen. Personally, I hope it will teach me that I was wrong with my skepticism.
I'm not sure why i'm replying here. Guess i'm bored.
> Time will no doubt teach us all a lessen.
I doubt it. You need to actually have a position that can be shown to be true or false with the passage of time before you can learn something from the passage of time. You have a bizare, logically disconnected, rant that does not make any predictions. I don't think any course of events would prove you right (or wrong).
> You may want to reevaluate your knowledge about the rest of the world
In context, we were discussing afluent countries, canada europe, etc.
> Also, that vaccine probably won't cost "just" $40 equally for everyone.
They will cost $0 directly. As you say there will be indirect costs based on taxes. However that will be true regardless of if you get the vaccine and be scaled based on your income, so im not sure how you think that applies to your argument sbout class divide.
Needs to be repeated again & again:
"Governments have no money of their own, it's citizens' (past, present and future - mostly the latter these days) who provide the cash via taxes".
This changes nothing. If anything it is wise for goverments to pay for vaccine because that means that economy will no longer be stifled by lockdowns and that means more money in taxes.
In any cases many governments already said they will provide vaccine for free.
Price is not an issue for rich countries. 500 Million vaccines for USA leaving kids and some other out...cost, what $25 Billion? Peanuts, compared to the damage it did /can do. Same for USA, EU, Japan, CA, Australia etc.
Poor countries are hit by covid-19 as well. Those folks deserve a vaccine too. Even if you don't care about the Humanitarian side of this, the west benefits from that directly by not having giant reservoirs for the virus.
Plus, they travel to the rich countries.New vaccines are coming in. China will probably use their own, India will copy one and costs next to nothing. Donations will make sure everyone has one.
My understanding is that they actually haven't tested at anything but -80C, and that it is potentially possible that it could be stored at higher temperatures, but it hasn't been examined yet.
Dry ice is very common, and you get 5 days at refrigerator temperature. Everywhere in the world is reachable in 5 days if you need to. It gets really expensive to charter flights to many areas, but it is possible if you have money to burn.
Of course we now have reason to believe that vaccines that don't need dry ice will be approved, so logistics will direct the easier to ship ones to remote places.
You can reach everywhere in 5 days but that's not enough. People have to come and get it, there's also a chance there will be a slow start due to concerns over a new drug that the media may emphasize was "rushed". Then there's the logistics of scheduling so many people. If you don't bring yourself a cold storage freezer you're committing to using 100% of your doses within 5 days which may not be possible.
For the first few months all doses will go to high risk people. Most won't have the option to refuse it.
Eventually you are right. If the Pfizer vaccine is to be used in remote places the people getting the vaccine will need to schedule it in advance (and probably pay for it) to ensure that once it arrives it is used.
It is, especially for far flung places. This stable vaccine will be very useful in places like the pacific islands, where air transport isn’t always an option.
Any island that doesn't have air transport doesn't really need the vaccine (if transit take weeks, infections on ships burn out before they get there).
Realistically, every major population can be reached in 24 hours by modern transport, and the Pfizer 5000-dose transport package keeps the temperature for 5 days.
mRNA is a term from molecular biology [0]. "MRNA" is the stock symbol of Moderna [1]. Both Pfizer/BioNTech and Moderna use a mRNA based method for their vaccine.
You might want to update the comment to avoid confusion.
The key differentiator is the mechanism of action, not the storage system.
The other two current candidates are mRNA vaccines, an approach which hasn't been used in humans before -- looks like the harbinger of a revolution but we have no past experience.
This O/AZ uses the actual spike protein embedded in a simian virus (that does not affect humans and has its own DNA removed). It's possible to generate antibodies to the vehicle (virus) which is why a simian virus is used (humans won't already have encountered it) but also means your own immune system could target the vaccine itself. Loewe speculates that this is why the higher dose was less effective.
The storage system is important and a key differentiator, tons of countries cannot effectively distribute a virus at -70° to population in the most vulnerable spots. I don't know why you felt the need to be so dismissive.
I am dismissive because distribution is not big-H Hard. It consists of known unknowns and can "simply" be solved by application of money. Yes, actually it's a systems problem: there is not infinite money, there are political interests. But compared to the science the problems are well understood.
On the other hand we still have no idea how well these vaccines will work. First, we have (as I discussed) two different approaches in the three current candidates, one of which is fairly new and one which is completely novel. We have had only limited time to see how well they work and have only limited experience in broad efficacy, duration of effect, and, crucially, how long they last (it takes a long time to learn if you'll need a 10 year booster!). We don't know how fast the virus mutates away from the vaccine's target (though we do currently think we have a good idea). And we simply haven't tried enough people to get a good handle on side effects.
One of the difficulties in solving these is that new approaches contain unknown unknown. Look at CRISPR-CAS: got a (deserved) Nobel this year yet may already have been discovered to be ineffective or worse in the real world. That takes time to learn.
Now it's not that the people doing the work are idiots -- they know all these problems better than I do. But I am appalled that this is treated by the press as a distinction between, say, a pair of beta implementations of something, one in Python and one in Ruby.
Going back to systems issues: when we don't know these factors we take a calculated risk (really an estimated risk). The social aspects of vaccination (close to ubiquitous use, the risk of any side effects increasing the anti-vaxx rate for other immunizations, which itself could become a public health disaster etc) mean these factors are upmost in public health officials, not whether they have adequate refrigeration.
Vaccines are particularly difficult for reasons like these above -- there's a reason why they have their own special laws and government-assumed liability insurance. I haven't worked on vaccines, so take this as you will, but I have worked in anti-invectives, have designed preclinical and clinical protocols (including first-in-human) which were submitted and approved by the FDA, run clinical trials, have presented to the FDA and defended protocol design, so I have some idea what's involved and how to read the presented endpoints and findings.
What does this imply? Is the approach by Oxford worse, or just more well known / less surprises? Does this mean that dosing the vaccination is somehow more difficult?
I'd argue that it is more accessible to everyone including developed nations. It only requires a standard technology freezer - like that you have in a residential home. COVID-19 has already cost the UK hundreds of billions, so being able to roll out a vaccine with minimum hassle and without needing specialist storage and training on its handling, is an absolutely enormous benefit.
Honestly I feel like this vaccine is going to leave the mRNA-based vaccines trailing in its wake in terms of global government adoption.
Moderna vaccine also seems to have similar storage requirements with a high price tag. BioNTech otoh has impractical storage requirements for the third world. AstraZenca's price and storage combiation may open possibilities for distributing this globally.
An important fact that I haven't seen mentioned in this thread is that 3m doses have been manufactured already and are available in the UK supply chain today. "All" that's required is the approval from the regulator - but I guess that is still a little way off. 3m would do a lot of good though - frontline staff, the most vulnerable, hotspots....
> Currently, OWS is working with 11 drug manufacturing companies to produce 800 million doses of six different COVID-19 vaccines, five of which are in Phase III clinical trials. By prepurchasing and premanufacturing these vaccines prior to approval, the vaccine distribution plan can be activated and supplies delivered within 24 hours of any of the vaccines receiving FDA approval.
3m worth of working vaccines would do a lot of good, the problem is we aren't sure it works (or even that it doesn't harm you or make you more susceptible)
Efficacy has been proven to a high enough degree of certainty that these vaccines are now being submitted for approval. Safety was largely proven in Phase 1/2 trials (before tens of thousands of people were injected with the stuff for Phase 3 trials). And all signs continue to show the vaccine to be safe (and data will continue to be collected for at least a year or two for the various Phase 3 trials).
Maybe "you" need more data for whatever concept you have in your head of how this should work. However, within the scientific community involved with developing and approving these vaccines, the data we have is sufficient (pending review of course).
Moderna and Pfizer submitted for approval shortly after they released their initial Phase 3 results. Approval is expected to be expedited, but will not be instant (I've read a few weeks, assuming no problems). Oxford/AstraZeneca will likely follow the same course now that their results are available (they were waiting for enough people in their trials to become infected, same as the other Phase 3 trials).
It is widely expected that large scale distribution of these vaccines will begin in late December.
Is this some attempt at a "gotcha"? It's all over the news, I'm sure you can Google it. CDC Director just said first vaccines should got out second week of December.
70% efficacy at 2c-8c storage for $4 is indeed excellent but many comments here go to "but modena is 95% efficacy whyyyy" and "they're underselling it"
I would far rather we report 70% and find its more effective than we report is up to 90% effective but in field deployment find its less. A 70% vaccine at wide scale release can keep R under 1.0
1/5th the price, and no need for freezers. This vaccine is huge. I pray for more like this.
I would far rather we report with just the tiniest bit of nuance. They did distinct variations for a reason. Nobody is reporting all the other approaches that were less favourable.
That makes no sense since there are no tested regimes with 70% effectiveness. The reporting should say there is a vaccine regime with 90% effectiveness, and add a footnote that another regime that will not be used had a far lower rate of effectiveness.
There is nothing on offer here with 70% effectiveness. There is a vaccine regime with 90% effectiveness. That's more than sufficient to be effective at ending the pandemic.
Thee's another regime that we can all just forget about because it uses the same vaccine but with a different method of delivery that will be discarded in favor of the method proven far more effective. Averaging the two makes no sense.
It's interesting to layman's eyes that the dosing regime using 1.5 doses is more effective than the one using 2 doses as I would expect the inverse; are there any plausible explanations for this?
These stats are based on 130 people getting covid out of an experiment of 25,000 people. They dont give a breakdown of the stats (e.g. who was on placebo, who was on which dosing regimen
) but those are small nubmers.
I think its possible that this is just noise. The difference between '60%' and '90%' might just be a handful of cases.
They show that it works though, thats the main thing.
edit: e.g. of those 130 cases lets assume half were in each regimen experiment. So 65 cases in the 'two full doses experiment' if they got 60% efficiacy then that means about 26 people with the vaccine got covid vs 39 with placebo. In the 'half dose then full dose' experiment if they got 90% efficacy then that means about 7 people with the vaccine got covid vs 58 with placebo. So the difference between 60% and 90% is 19 people. They show that the vaccine works but there is lots of uncertainty between the two dosing regimens.
It's because of the way the AZ vaccine works. It uses a different virus to infect cells which then create the antigen to stimulate the immune response. These are a bit unstable, since the vaccine itself, being a virus, is an immune system trigger. The immune system might snuff out the vaccine itself after a huge first dose, then the second dose is wiped out.
This is I think why the mRNA vaccines are doing better. They don't use a virus as a vector, they use a less convoluted vector of a more basic mRNA instruction set. They're also in a way more "scalable" in that a future disease or a mutation of Covid with a new spike protein could have a new vaccine made quickly by tweaking the mRNA sequence.
One theory is that it's due to the vector. This utilizes an adenovirus (which has been used more commonly in vaccines previously, and is different from the novel mRNA viruses developed by Biontech/Pfizer/Moderna). The thought process is that with a larger initial dose of the vaccine, more immune resistance is built up by the body initially, which then neutralizes some of the booster when its given later.
We (Britain) may have totally screwed up our general response to COVID. But at least we’re still pretty good at science. Thanks Oxford for saving the day.
Tyler Cowen made this point a few months ago (https://marginalrevolution.com/marginalrevolution/2020/07/wh...): the public health response has been "generally poor" but the UK was first on the mark with dexamethasone and has been among the first with the vaccines. He went as far as saying the UK has had the best response to COVID despite the public health response.
So, a member of my immediate family is senior management at Public Health England, the civil service institution that should have been planning for this.
When the government announced they were shutting down PHE, in an attempt to copy the RKI (forgetting that PHE is far more than disease control, of course), the RKI wrote a letter to all senior management at PHE. This was quite a confused letter - the RKI didn’t understand why the UK gov were making this decision, when the RKI modelled their processes on PHE. I’ve read the letter.
Add to this, daily squabbles between cabinet office and other branches of government. If there was good news, you’d hear back immediately and you’d be blocked from sharing it. Bad news, cabinet would stall sometimes for weeks.
But ultimately all the guidance was irrelevant because the UK government are not interested in listening to it. When an adviser egregiously broke the rules, a story which dominated the headlines for weeks, they changed the rules. You see it now - the UK isn’t even on the downslope of wave 2, but apparently in 2 weeks we’ll have fans at football games and business as usual.
Also worth noting that we did this by having a board research base that was not tied to immediate returns. A year ago Sarah Gilbert was struggling to get funding for work on the MERS vaccine, which was seen as largely irrelevant.
Not to downplay Oxford or Britain's work, but I think it's safe to argue that the poor general response to COVID is also an indicator of your skill at science. And I say this as American, who's response was just as bad or worse.
People are going to look back at this pandemic with amazement at the work the world scientists did to create a vaccine in record time, but with shame and embarrassment at the loss of life in countries that are considered world powers due to politics, ignorance, and stubbornness.
> it's safe to argue that the poor general response to COVID is also an indicator of your skill at science
This isn’t safe to argue at all. In fact, it’s completely wrong. We know that the poor UK response is almost exclusively due to politicking and government corruption. The scientific advisory panel of the government (SAGE) hasn’t always been right in their assessment but they very quickly produced rigorous working models and solid recommendations, most of which have mirrored (and continue to mirror) the international consensus. Furthermore, public research in the UK has, sometimes against the active opposition of the government, done stellar work to ramp up testing and genetic sequencing.
For instance, several institutes (incl. the Crick Institute in London and the University of Cambridge) had extensive testing capabilities set up in record time, but their offers to official channels were ignored for weeks, if not months (the Crick in particular simply ignored this and already provided testing internally and externally, at a time when basically no country had widespread testing yet).
Likewise, a collaboration of different institutes quickly set up genome sequencing pipelines for COVID-19 samples, and as far as I know the Sanger Institute is sequencing more COVID-19 samples than any other individual entity in the world: https://www.sanger.ac.uk/about/who-we-are/sanger-institute/t...
> but I think it's safe to argue that the poor general response to COVID is also an indicator of your skill at science.
That's not logical at all. It's a reasonable argument that poor general response to COVID is an indicator that you aren't currently doing a good job of governance, but that's a whole different kettle of fish.
This statement seems a big deal:
"There were no hospitalised or severe cases in anyone who received the vaccine"
Is that also true of the Pfizer and Moderna trials?
Are the various trials measuring 'effectiveness' in the same way?
Is there a standard for 'effectiveness' in these Covid-19 trials?
It will take some digging and real effort to compare the risks and benefits of the various vaccines coming to market.
This is the information we have on the BioNTech/Pfizer vaccine regarding severe cases: “There were 10 severe cases of COVID-19 observed in the trial, with nine of the cases occurring in the placebo group and one in the BNT162b2 vaccinated group.”
Just as a reminder, that vaccine had more than 40k people in each group, with 170 cases of COVID-19 being observed, 162 in the placebo group, 8 in the vaccine group.
As you can see, the sample sizes get quite small, so I’m not sure how much, if anything, this tells you regarding severe cases. There could have been just as well no severe case in the treatment group, just by luck. What would that tell us?
I didn’t find any info regarding severe cases and the Moderna vaccine but I maybe I missed it. Those press releases are hard to read.
It's about 43k people total, not per group. And I think this was a multi-arm study, they're testing two variables across two population groups - here's the study paperwork:
Everybody in all arms (groups) gets a jab, twice, but what exactly what is in the needle varies. The study paperwork doesn't say which placebo was used in this trial (the participants would definitely have been told), sometimes vaccine studies use a vaccine for something else that you didn't need but is presumably harmless (e.g. think of vaccines you take when going somewhere a bit dubious on holiday). Other times they just use saline. Some other groups got higher doses of vaccine.
Anyway, since everybody got stabbed, nobody (as much as possible not even the people giving you a jab) know what's in the needle - everybody gets assessed for side effects. One of the very revealing things about all these studies is how many side effects you get for injecting people with saline. Sore arm makes some sense at least, somebody stuck a tiny needle in your arm - but you'll get headaches, dizziness, flu symptoms even. The mind is powerful.
Seems like the sample size is probably too small to draw any conclusions there. 131 got covid in the trial, if 70% effective than 39 should be from the group that got the vaccine (i think. Did i do that right given they're combining the two dosing regime)?
Maybe its chance that none of those 39 got really sick. I'm not sure what the age breakdown of trial participants was- were the people in the oxford trial younger? Did the distribution match the distribution from the mRNA trials? I have no idea.
(afaict) You're right about the 39 (risk reduction = 1-39/131 ~= 70%).
But you're less correct about saying "smple size is probably too small" (in general, people really really really need to stop dismissing things based on sample sizes until they actually go through a Power calculation!). Your question about demographic breakdown is entirely valid.
Hospitalization rate for covid is about 228.7 hospitalizations per 100,000 population [0]. Or, more easily interpretted, about 10-20% of cases turning to hospitalization.
Taking the more conservative (10%) rate, we'd need 31 samples for a 95% CI and 5% margin of error. Thus, the interpetation is that is it unlikely that the _lack of seeing any hospitalizations in the vaccine+covid-positive group is by chance_.
Thanks, this is a good point. I just blindly assumed it was too small because it was a small number.
I think there was a bit of an implication in the parent post that it would eliminate hospitalizations (instead of just reduce), i still think that is unrealistic.
I don't think it's fair to say " that is it unlikely that the _lack of seeing any hospitalizations in the vaccine+covid-positive group is by chance" until we see the demographic breakdowns. The difference in hospitalization likelihood between demographics is too big to ignore.
> Is that also true of the Pfizer and Moderna trials? Are the various trials measuring 'effectiveness' in the same way? Is there a standard for 'effectiveness' in these Covid-19 trials?
Yes, its true that there were no "severe" cases in the other vaccine trials as well.
> This statement seems a big deal: "There were no hospitalised or severe cases in anyone who received the vaccine"
It may be. When considering disease severity, we are no longer looking at a pool of people who have been given the vaccine (which is in the tens of thousands for all of these), we are looking at a pool of people who got sick. That means the sample size is reduced to approximately 90-100 for placebo wing of each vaccine, and 30 for ChadOx vaccine arm, and about 5 for Moderna/Pfizer vaccine arms each. That's fairly small.
Seems like the estimated rate of severe cases is around 10-20%. Assuming its 10% (which would mean its harder to identify an actual reduction in disease severity rate from the placebo group), then in the case of Pfizer/Moderna, there would be a greater than 50% chance of seeing no severe cases in a group of 5 infected, vaccinated patients, even if there was no effect on the severity of the disease. The greatest benefit to the vaccine is that they seem to prevent infections substantially, but that also means it will take months before enough infections occur to get some kind of statistical significance on if severity is also affected.
But with this vaccine, 30 cases with no infections is definitely in the realm of statistical significance. I don't have the exact numbers from the trial, but if it indeed is 0/30 vs around 10/100 between the vaccine/placebo wings, it definitely meets the typical thresholds of statistical significance.
It's important to note that, at least according to my understanding, the Pfizer/Moderna trials are measuring symptomatic cases, not doing actual tests on their trial participants. This means that it could well mean that the reason the vaccines appear to be so effective is because they truly are reducing the severity of the disease to the point of being asymptomatic. We just aren't able to see it yet due to the way the data is being collected.
So, the Oxford vaccine stated "... no hospitalised or severe cases ..."
The Pfizer press release states:
"There were 10 severe cases of COVID-19 observed in the trial, with nine of the cases occurring in the placebo group and one in the BNT162b2 vaccinated group."
So, zero severe cases for Oxford, and one for Pfizer.
Interesting.
Should also point out the Pfizer trial may have had 43,000 participants, and the Oxford one 24,000, so they are different size trials.
Also, it's super easy to miss important details when comparing outcomes like
this, to do this properly really requires a project or in-depth investigation,
not my 15-minutes research effort. :)
"So, zero severe cases for Oxford, and one for Pfizer. Interesting." What is interesting? That they probably both have the same rate, and we are seeing a statistical fluctuation because of the low sample number?
The statistical difference between 25,000 and 43,000 samples being... small. Basically, any effect visible at less than 2 in 40,000 might be missed by the 25,000 test.
Seriously, do you think this is a huge difference in quality of measurements?
There were no hospitalisations or severe incidents for either the Pfizer and Moderna trials were was related to the vaccine.
And it's pretty easy to compare the vaccines. It will mostly come down to price, ease of manufacture and ease of distribution i.e. temperature. Given that for the 3 viruses all have no risks associated with their use.
> There were no hospitalisations or severe for both the Pfizer and Moderna trials that was related to the vaccine.
I think the commenter wanted to know whether anyone who received the vaccine was hospitalized for anything covid related, not for anything vaccine related.
Only in the richest countries. Due to the totally different age pyramid and thus few severe cases, vaccination might not be worth it for the poorest countries even at this lower price.
Lockdown/social distancing hurts the economies everywhere. India and south east Asia has a huge population of street vendors that depend on buyers being out in the streets.
We don't for absolute certainty, but there's no reason to think there would be. Consider:
a) A virus that is known to cause severe disease in a significant proportion of people, including months-long serious health effects, hospitalisation and death.
b) A virus chosen because it doesn't causing any ill-effects in humans, modified to take on some non-harmful aspects of virus a) and found to not cause any significant harm in tens of thousands of people over several months.
Which is more likely to cause long-term side effects?
And not only that but option (b) is a virus "that has been genetically changed so that it is impossible for it to grow in humans," according to the article.
We can't. If everybody turns into superheros in 10 years, we wouldnt know; or maybe this is actually the backstory of 'children of men'; we can't know. RNA vaccines are researched in animals for about a decade, but long term effects are usually not beeing found in such studies (disection usually cuts that short). There is though no theoretical nor experiental evidence for that.
Most adverse events (narcolepsy and GBS included) occur within a few months (1-3) of administration. The fact that some are reported after years doesn't mean they are "long term": it only means it took a while to vaccinate those people.
So far none of the trials (even more so AZ) has incurred in vaccine-related adverse events of this sort.
If there is no known mechanism by which side effects could occur with long gestation, and if experience with other vaccines and vaccine trials provides no evidence of any such, then it would seem unlikely.
There was one vaccinated but then severe case in Pfizer trial out of 170 cases evaluated where placebo-then-ill cases are included, or 1 from total 8 vaccinated but then ill.
“There were 10 severe cases of COVID-19 observed in the trial, with nine of the cases occurring in the placebo group and one in the BNT162b2 vaccinated group.” (1) “170 confirmed cases of COVID-19 were evaluated, with 162 observed in the placebo group versus 8 in the vaccine group.”
Here [1] it says the vaccine was designed mostly over the weekend of 11th Jan 2020. Here we are 10 months later and we know it works. If our knowledge of vaccine design is so good experts can design a vaccine that works over a weekend, what new breakthroughs are required to reduce the time between then and now substantially? A lot of benefit could have been had if we'd been able to get along this path more quickly.
Definitely. It’s a similar situation with the aviation too.
Unfortunately, rules in fields like medicine and aviation are written with blood. Someone gets too greedy or too comfortable and you have large numbers of people death or incapacitated.
We already have large numbers of charlatans preying on the hopes of desperate people, must be very careful not to lower the barrier too much or these might jump too. Even worse, people might be targeted by slick psychopaths and coerced into extremely dangerous things, destroying communities when anything goes wrong.
Hopefully though, some mountains might have been moved and some things might have gotten faster from now on.
It's not about following arbitrary rules for the sake of following rules.
There are people out there that won't hesitate to kill any number of people for the hard cash or fame, some did it before and that's how the rules were born. I am sure that some of rules could be revisited thanks to the new tech but portraying it as "rules kill people" is intellectually dishonest or naive.
Look what happened with Boeing 737-MAX. Some businessmen, scientists and engineers will cut corners to get their job "done" and every now and then it will be catastrophic.
Challenge trials. https://www.1daysooner.org/ If it were considered ethical to do them, we could have known in a few weeks. "Medical ethics" claims another million lives.
We've subsequently learned that even young healthy and initially asymptomatic people can become permanently ill from so called "long COVID". The ethicists were right to say no.
People join the military not knowing whether or not they will ever go to war, yet they still join. By doing so they risk death, dismemberment, and all manner of long term disability under the belief that doing so makes everyone else safer.
If exposing a few people on purpose is a moral wrong, then surely allowing millions of them to contract it by accident so that a few people in your RCT can become infected by chance is a moral abomination.
A traditional trial requires you to wait for the pandemic to spread in order to get enough positive people in your trial for significance. It's effectively like "challenging" random people in the public in the hopes that some of them are in your treatment group.
The people and government organizations that opposed challenge trials are preventing the participants in challenge trails from saving people who actually did die from Covid.
I'm not sure that's correct as the safety data had been the last to come in. You still have to run a large phase 3 trial to collect safety data, challenge trial or not.
This makes no sense to me. Preventing challenge trials causes more people to die and become permanently ill. What ethical system are you operating under where that is morally preferable?
FWIW, ethicists were split, but mostly on board with HCTs. It was mostly the government that was opposed.
IIRC, we were fairly unaware of the long term effects at that point. All we really knew was that age had a factor. So a bunch of healthy young people would have signed up, thinking that the chances of harm, even if they got the placebo, were fairly low, when in reality there were significant chances of being permanently (or at least very long term) maimed.
Essentially, no one signing up for the trial would have been properly able to give consent, because no one knew the real consequences.
Nobody knew what the long term effects were, but we knew that there was uncertainty about them. Informed consent doesn't require perfect information. Just the best possible information, and a fair appraisal of uncertainty.
As a young and healthy challenge trial volunteer, who is now watching the panic metastasize into an existential threat to free civilization, no they were not. Blocking these trials is the worst miscarriage of ethics that I have ever seen.
The point that challenge trials don't determine safety is accurate, but most of the article is again arguing about the ethics rather than the efficacy. Imagine if volunteers were not permitted by ethicists to storm the beaches of Normandy because their safety could not be guaranteed.
Our current testing protocol requires letting the virus rampage through the population before the trials will achieve statistical significance, which is surely more unethical than deliberately exposing a small number of people.
I tend to agree in the case of Covid, but I'll play devil's advocate...
Suppose we replace Covid with "car crashes" and vaccine with "seatbelts". This is a good analogy because crashes are rare and we can't cure trauma (like on Star Trek). It would be absurd to deliberately cause car crashes in order to study the effect of seatbelts. For the experimental group, there will still be some minor injuries. For the control group, many will die.
That sounds more like doing challenge trials for an ebola vaccine, for which I'd expect you'd get very few volunteers. Still though, if there are people willing to risk sacrificing themselves, and the information would definitely save lives, we should let people do that for the greater good. The world's militaries throw away far more lives for far less benefit.
Even once safety is established, our current protocol requires waiting for wave of infections to sweep so thoroughly through the population that some of the study volunteers are infected by chance.
That's incorrect. Both are determined from the same tests and determining safety takes longer.
Phase III trials for each of these new vaccines end long after the efficacy is determined. Estimated primary completion dates are in June 2021 (BioNTech/Pfizer) and November 2021 (Moderna).
Even after the drug is accepted, monitoring for safety continues.
Nothing. Timelines for Covid-19 vaccine are already compressed. Even this data is just preliminary from Phase III.
Limiting factor is safety and testing for safety.
They started trials with two people, one gets vaccine one gets placebo. They look for side effects then add more and more people while constantly observing those vaccinated for side effects.
Vaccines are not inherently safe, they are safe because they have gone trough huge amount of volunteer testing. If there are unwanted side-effects, vaccine is withdrawn. Since vaccines work with the immune system, you must look for autoimmune reactions, neurological symptoms etc. Some of them can emerge weeks or months later. With new mRNA vaccines there are even more unknowns.
Emergency authorization they seek means taking calculated risk. With covid-19 epidemic taking that risk is acceptable.
I cannot think of a valid utilitarian argument allowing willing people from getting a vaccine.
First, vaccines have an extremely high success rate, 33% of vaccines make it through all trials to approval. 50% after phase 1 is complete.
The worst vaccine side effect ever is widely considered to be the swine flu vaccine from 60 years ago, where 1 in 100,000 got GBS (a bad disease).
If we knew with 100% confidence that this vaccine was tied for the worst, then if you are over 65 it would be about 1,000x better for you to take this "bad vaccine" versus not.
Each successive trial lost us a lot of time, and very little confidence gain.
The reality is we had many groups all independently find a vaccine that worked in Q12020. It's only the government ban on their use that allowed the pandemic to proceed like it has.
Right now in the US, the FDA has said it is not even planning to MEET on the Pfizer candidate's approval for 3 weeks. Just insane. Then, the CDC says it needs 24-48 hours after FDA approval to authorize it's release. Why can't the meet right now? Why can't the CDC pre approve release? Or be in the meeting and give simultaneous approval? Or be on a phone alert to give approval within 1 hour?
The most likely answer is that in a nationally declared pandemic, any vaccine produced by someone who has gotten a vaccine approved in the last 10 years can sell and distribute (cash only no insurance) vaccines without approval. Require them to collect data on its usage and efficacy. Wait until normal process to require people to be vaccinated.
>I cannot think of a valid utilitarian argument allowing willing people from getting a vaccine.
I think you should check your math. Because covid-19 infection fatality rate is "relatively low", only 10 times seasonal influenza (3X for people in their 30's 15X for people in their 70s) the limit where utility turns negative is quite low.
One purpose of approval is to move responsibility from drug companies to the government. They can just pay small fee for National Vaccine Injury Compensation Program or something similar. If you allow volunteers but they have to pay the insurance from free markets, vaccines become too expensive. Drug companies are not willing to give them.
>The worst vaccine side effect ever is widely considered to be the swine flu vaccine from 60 years ago, where 1 in 100,000 got GBS (a bad disease).
During the 2009 A(H1N1) influenza pandemic Finnish health system used vaccine called Pandemrix, It was almost exactly the same as Focetria used elsewhere in the Europe but it was manufactured using slightly different method. It caused Narcolepsy for 200 kids in Finland and 100 in Sweden before withdrawn.
Thanks for responding, I am genuinely curious if my math is wrong so appreciate the discussion.
First, regarding "worst case side effects", I am willing to accept your premise that elevated rates of narcolepsy was in the 2009 A(H1N1) vaccine was worse, and do some math based on that.
If you assume that people had a 10% chance of contracting the disease, you can say that those over 75 would have approximately a 0.46% chance of dying (4.6 in 1,000 dead) if they don't get the vaccine.
If they do get a vaccine, that turns out to be as bad as Pandemrix (I believe your example of the worst case side effects), then you would expect 1 in 18400 to get narcolepsy. (source: https://en.wikipedia.org/wiki/Pandemrix).
So if you are a regulator looking at the elderly population, and you assume this is tied for Pandemrix, then for every 18,400 people you would assume 1 case of narcolepsy if you give the vaccine, and 84.64 dead. (85x by volume).
I don't know your opinion of "how much worse is death versus narcolepsy?". If you believe death is 10x worse than narcolepsy, then by severity and volume, taking a vaccine with the worst side effects ever would seem about 850x better than not taking it (in elderly populations). Earlier in the pandemic, when IFRs were over 2x as bad, this was well over 1,000x better.
If you are getting different math, please let me know, because even using Pendemrix, I cannot seem to justify banning vaccines on utilitarian grounds.
Now I do agree that moving responsibility from drug companies to the government is fine, but I think that can be addressed directly if that is a concern. If the argument is "without government assuming responsibility they would be too expensive", I don't think we have any proof of that, not enough for a ban.
None. We could have run a 400 person challenge trial in March and gotten the effqcoty data then deployed to Healthcare workers and surveillance for safety. This would entirely change the situation we're seeing now.
It would require forgoing any kind of serious trials to determine the efficacy and safety of the vaccine.
It is the classic "make a baby in 9 months with 9 women" dilemma. There is no way around conducting a trial and waiting long enough until you see what happens to the participants.
None. Longitudinal trails are required to assess safety - literally waiting and seeing what happens. There's no other way to assess long term effects on the human system. For the avoidance of any doubt none of the new vaccines have had anything like the proper amount of time for a bare minimum longitudinal trial. Whether you decide to take a vaccine nobody in the world is more than 6 months out on will hopefully be left to personal choice.
The main bottleneck is getting a bunch of volunteers, vaccinating them, and seeing how many get the disease over the next few months. Kinda hard to speed that up, unless you're confident/desperate enough to just skip testing. Maybe if the disease were 10X more dangerous and you had a vaccine that was just a minor variation of a previous one, it'd be worth it.
A little time could maybe be shaved off by speeding up production. The mRNA vaccines have an advantage here, you can basically use an RNA printer to churn out whatever RNA sequence you need.
Correct me if I am wrong,
Oxford uses traditional Vaccine design technique (using a weaker virus and adding spikes or something similar) while Biontech(Pfizer) and ModeRNA use MRNA which is completely new technique (messenger RNA).
This is awesome for more than just vaccinations. Traditionally the groups allocating govt funding to science and industries are very risk averse and this could be one more example where taking risks can payoff.
I thought adenoviral vaccines were also relatively new. Not as new as mRNA which is bleeding edge, but still i think this would be the first time this technique would be approved for human use should it be approved.
If I remember correctly, the Ebola vaccine is the first approved vaccine to use another virus as a vector. The first one to be approved (by Merck) does not use an adenovirus, but the second approved one (by J&J) does.
Note that approvals of these were late 2019 and the summer of this year. So still very new from an "approved on humans" point of view (although not _as_ new as mRNA-based vaccines). The techniques have both been in development for years and years of course, including determining their safety profiles.
That statement is somewhat ambiguous, because there have been vaccines against adenovirus infection available since the 70s, but the use of adenovirus as a vaccine vector (which us different) is fairly new. The latter has not been the case for "decades".
> One dosing regimen (n=2,741) showed vaccine efficacy of 90% when AZD1222 was given as a half dose, followed by a full dose at least one month apart, and another dosing regimen (n=8,895) showed 62% efficacy when given as two full doses at least one month apart. The combined analysis from both dosing regimens (n=11,636) resulted in an average efficacy of 70%. All results were statistically significant (p<=0.0001).
Also:
> and no hospitalisations or severe cases of the disease were reported in participants receiving the vaccine.
“The thing is, the immune system is very complicated.”
quote from the link here, but for those who don’t want to click through (this article is fascinating though), it is told in the context of a joke which i will post below the link.
There’s a joke about immunology, which Jessica Metcalf of Princeton recently told me. An immunologist and a cardiologist are kidnapped. The kidnappers threaten to shoot one of them, but promise to spare whoever has made the greater contribution to humanity. The cardiologist says, “Well, I’ve identified drugs that have saved the lives of millions of people.” Impressed, the kidnappers turn to the immunologist. “What have you done?” they ask. The immunologist says, “The thing is, the immune system is very complicated…” And the cardiologist says, “Just shoot me now.”
IANAD but my guess is maybe a stronger immune response in the first dose makes the immune system respond so quickly to the second dose, that it doesn't have time to get anywhere and interact with enough of the body to have much of an effect. That way a weaker immunization in the first dose leaves more room for the second dose to have a refreshing/strengthening effect. Basically, 1 + 2 > 2 + 0
This vaccine is an inactive host virus whose payload has been replaced by the coronavirus "spike". It has always been a worry that the body will generate immunity to the host virus and thus make the vaccine less effective. That is a likely explanation for the first-full-dose regimen being less effective.
One thing that isn't obvious to me is exactly how `n` is defined, and how that relates to how many people of that `n` were infected by covid during the trial. E.g. maybe n=2,741 people were vaccinated following the first dosing protocol, but perhaps only a small fraction were infected with covid. So the actual sample sizes being used to estimate the efficacy of each dosing protocol may be smaller.
However, mRNA vaccines require low temperature storage and are in general harder to handle. This translates to additional cost in production, throughout the logistics chain and delivery.
Pfizer are also working on a lyophilised, aka freeze-dried, version of their vaccine, which would not need to be stored at -80 C. This is from July [1], not sure if there is any more news:
> But we also hope to have, as we always do in life cycle management, a new lyophilized formulated vaccine by -- within maybe a year after initial delivery such as fourth quarter 2021 and the lyophilized formulation could be stored in refrigerator.
I think it's likely that they'll need to be distributed frozen, but there's a lot that can be done researching preservatives. The the moderna vaccine is higher temperature than the pfveizer one for this reason.
no real idea, but my guess is that its likely true that mRNA fragment production is cheaper, but inactivated vector manufacturing is already scaled up and out globally and mRNA is not-- existing labs around the world can maybe be more easily equipped to scale up production?
Not for developing countries. And ultimately it is important for them to get vaccinated too, otherwise they will form a huge reservoir of COVID that will inevitably mutate and come back around to us.
That is not how it works. The Spanish Flu hasn't "come back" yet and coronaviruses mutate a lot more slowly. It couldn't really come back anyway, because it's still there, downgraded to regular flu.
Your example proves exactly the opposite of the point you think it does. Every year the flu virus comes back slightly mutated, and the immunity process starts all over again. In the summer the southern hemisphere acts as of reservoir of the virus and vice versa in the winter. This exact process could happen with COVID too. You are right that it does mutate more slowly, but there are upwards of 4 billion people in these countries. A very small number times 1 billion is still a much larger number.
I believe you misread the abstract. After reading the whole article, I believe it should be "include the `2009 swine flu pandemic`, as well as the `Spanish flu`".
That headline is not quite correct. From the article:
> Phase 3 interim analysis including 131 Covid-19 cases indicates that the vaccine is [on average] 70.4% effective when combining data from two dosing regimens ... In the two different dose regimens vaccine efficacy was 90% in one and 62% in the other
And to be clear, it's not just one dose vs two:
> tests on two different dose regimens showing that the vaccine was 90% effective if administered at a half dose and then at a full dose, or 62% effective if administered in two full doses.
So "Oxford vaccine is up to 90% effective", perhaps?
Another article I read seemed to indicate they haven’t investigated the half dose regimen fully so it sounds like until more testing is done that’s not the recommended path (in which case the headline is being generous).
Is there any research or early guestimates about risks (or benefits) of getting multiple different vaccines for Covid? E.g. What if one gets this, and then later moderna vaccine? Will they fight each other, or work together or is it unknown whats going to happen?
I'm not a microbiologist, but this is not how vaccines work. The vaccines are going to put "something strange" in your body that "resembles" the virus, but it's not the virus (it's either a deactivated version of it, or some proteins which identify it...) and then is YOUR immune system the one which "attacks" this pseudo-virus. In this way, your immune system is learning how to defend to "this kind" of strange agents.
In a future if your immune system sees the virus, will defend you.
If you get the two kinds at the same time, maybe the two doses are too much for your immune system to handle it properly and the side effects may affect you (e.g. you can get fever because your immune system is under too heavy load).
"In the future your immune system may help the virus." I think they tested for this in the Oxford vaccine but there is an interesting case such as in Dengue where in a subsequent infection you may do worse with antibodies present. https://en.wikipedia.org/wiki/Antibody-dependent_enhancement
Most of the vaccines developed seem to work pretty much the same, by targeting the same spike protein.
And I am also far from being a microbiologist either, but I do know that the immune system is very complex, so I would not rule anything out, when messing with it.
In any case, getting the vaccination can (maybe) actually increase your risk of a severe Covid sickness, when you are exposed to real covid virus at the same time.
And I have no data for it and I can imagine it being hard to get reliable data about it, but autoimmune sickness is on the rise. I am not sure a quickly hacked together vaccine can rule that possibility out.
There are definitely benefits to vaccine diversity. The Oxford ChAdOx1 virus involves putting a modified chimp adenovirus into people. People don't have immunity to chimp adenovirus, so it infects them and delivers the spike protein, which elicits immunity. But that might also elicit immunity to the chimp adenovirus! If that happens, then a later does of the vaccine - say, for a new strain of SARS-CoV-2 in a year or two - might not be as effective, because immunity to the chimp adenovirus will stop the vaccine delivering the spike. In that case, having a different way to deliver a vaccine will be a life-saver.
Indeed. Maybe someone with more expertise can chime in — it's not clear to me if getting a vaccine with the chimp adenovirus backbone would preclude the possibility of getting another vaccine based on that backbone in the future (because of immunity to the backbone).
In case anybody was wondering what this actually is: “The ChAdOx1 vaccine is a chimpanzee adenovirus vaccine vector.” They put a corona spike sequence into it.
By comparison, the Moderna is making a RNA vaccine, and BioNTech an epitope vaccine (the actual protein).
The ‘invasive’ effect is decreasing in that order. Oxford’s ChAdOx1 infects your cells to create RNA, then protein, then T-cell recognition/apoptosis, then epitopes trigger B-cell antibody production. Moderna RNA skips the infection part. BioNTech epitopes go right to B-cells.
But, they also have deceasing stability and manufacturing scalability in that order.
> Our vaccine consists of a short segment of genetic material, called messenger RNA, that provides instructions for a human cell to make a harmless version of a target protein, or immunogen, which activates the body’s immune response against the SARS-CoV-2 virus
Thanks for the additional context. This is interesting because the has been some worry about the safety of the new and relatively untested mRNA technology, but this makes it seem like traditional vaccines are just that with extra steps. Should that be a license to feel safer about mRNA?
The press release is interesting. Not the best way to present their data. Immediate conclusion of many newspapers is "oxford vaccine is less effective then...".
Better that than to be seen to overstate its effectiveness. The worst case scenario is people refuse to take it because they think they're being lied too or manipulated in some way.
On the (BBC) radio news earlier only the 90% figure was mentioned, not the 70%. This differs from the BBC news website, which started with the 70% figure and mentioned the 90% afterwards.
Maybe. But it's also time to compete and current headlines are not working. If the public opinion is that it's far less effective then the other 2, what is happening now, you are putting the politicians in a difficult position that want to buy your vaccine. If you dig deeper you will find results for all vaccins are pretty similar. For instance even though one of the trials with Oxford vaccine had more people with Covid sypmtoms they had no severe cases, compared to one severe case with the Pfizer trial. And the total for both are too low to make definite conclusions.
Headlines shouldn't be manipulated to make life easier for politicians...
Also, the issue will not be which vaccine is chosen, but above a certain percentage of effectiveness who can even supply enough of their vaccine to meet demand?
Incoming possible Silly, Stupid and Lazy Questions,
1. Are there any vaccine ( of any Disease ) that are 100% effective? Or do we operate ( as I would assume ) something like 5 Nines effective rate and call it 100%?
2. Across all type of Vaccine, what are the average or median effective rate? i.e Should we expect Vaccine to be 90%+ effective in the first place? Or is that a wrong expectation to make?
3. What happens in the case of 10% ineffective, do they take a third dose?
Superficially regarding number 2: on a population scale a lot depends on how contagious the disease is. The measles vaccine is very efficient (over 95% after two doses), but still requires something like a 90% vaccination grade to prevent outbreaks. Measles is very very very contagious.
Covid is not nearly as contagious, so to prevent outbreaks it doesn't have to be nearly as good at the same vaccination grade.
For an individual, however, 70% would not feel very reassuring, which is why we need a lot of people getting vaccinated.
Edit: fixed some autocorrect issues. I feel I should add: measles is not at fun, even if you don't have any complications. You become very sick. Serious complications are _a lot_ more common than adverse reactions to the vaccine. Don't rely on other people being vaccinated unless you have a compromised immune system in any way.
> For an individual, however, 70% would not feel very reassuring, which is why we need a lot of people getting vaccinated.
Agreed, but keep in mind that no one in the Oxford trial who got the vaccine got a serious case of COVID or needed to go to the hospital. So it's only 70%-90% effective (depending on dose) at keeping you from getting infected, but so far 100% effective at reducing severity and keeping you from dying or going to the hospital. So that's a huge positive to keep in mind and yet another reason to get vaccinated.
On 1 : I think that measles vaccines have to be 95%+ effective, or basically you have no herd immunity to prevent an outbreak and protect (for example) infants not yet immunized. Because, measles is so amazingly transmissible. Other vaccines are much less effective (ie. yellow fever?) but because the diseases are harder to catch they can be suppressed in the population just as well.
The sort of polio vaccine used in rich countries is almost 100% effective after three doses. I did some spot checking of a bunch of vaccines I'd heard of and most seem to be between 90% and 99% effective so Covid-19 vaccines seem to be in line with expectations. The flu is worse but that's always a guessing game of which strain will be prevalent when they're making the vaccine. I think that's because more doses tend to be more effective and if a single dose doesn't get you there they just give you more doses, like the two doses for the mRNA covid vaccines. Effectiveness here is how many people get sick. You don't know in this circumstance that they're going to get sick until it happens, though maybe you could keep track of everybody's antibody levels compared to what they should be and guess. That would be way more expensive than just giving everybody the same schedule of doses though.
Not an epidemiologist, but I think the goal of mass vaccination if to make R drop to well below 1. If everybody is vaccinated with a 90% effective vaccine, then R drops by a factor of 10 (I think) so that sounds pretty good?
Yes, R is at 1.3 with WFH and other restriction. In March, R was 3-5 without restrictions.
If everyone got vaccinated with 90% effectivity (or even 70%), it would be enough. However, availability won't be sufficient to get to 100% within a year, and compliance seems to be somewhere around 50-70% at most given polls. (There are a huge number of people even in this forum who are antisocial - "I won't get vaccinated until I have seen super-long-term effects, and screw the people who I superspread the disease to".)
Antisocial? Let me decide about myself. How did it go, "my body, my choice"? Also, I find it interesting how everyone suddenly trusts 100% every claim made by big pharmaceutical companies, even though most of them don't have a good history. Volkswagen was also complying to all the laws and standards, until it turned out it actually didn't.
> 2. Across all type of Vaccine, what are the average or median effective rate? i.e Should we expect Vaccine to be 90%+ effective in the first place? Or is that a wrong expectation to make?
Sometimes, vaccines are only 30% or 40% effective, leading to terrible flu seasons.
I don't really know the mean/median/mode, but 90% is really high for a vaccine.
> 3. What happens in the case of 10% ineffective, do they take a third dose?
Yeah. Influenza is also a segmented virus. The RNA is composed of eight segments. The virus can produce new strains by shuffling segments between to different strains when a cell is infected by both. Influenza can mutate very quickly.
Simple single stranded viruses like Covid19 are vastly more stable. A good vaccine as long as we force everyone to take it will wipe out covid19.
The point of a vaccine is to give you immunity WITHOUT getting the virus.
Your immune system naturally becomes immune after it fights off an infection. But because of the risk of long-term effects and/or death when you're infected with COVID19, people want a safer solution that provides immunity.
A vaccine provides immunity, but at a lesser rate than the actual virus. But 90% (or even 70%) effectiveness is a good thing: it means 90% to 70% people do NOT spread the virus anymore.
You'd think that means 90% or 70% fewer deaths, but that's mistaken. That 70% is compounded over-and-over every generation. If everyone else is vaccinated: you infect 70% fewer people. Those people infect 70% fewer people, and those people infect 70% fewer people.
After 3 generations, a 70% vaccine would wipe out 97.3% of possible infections. And a "generation" in COVID19 terms is roughly 1-week.
---------
So yes, even a 70% vaccine (if everyone took it) is a very, very, very good thing. But the two vaccine trials that finished first were 90% effective, so I think people will prefer the higher-efficacy (at least, if they have access to Dry Ice / -80C storage).
1. Smallpox vaccine is 100% effective
2. 90% is high.
3. Probably not. Immune systems are weird and incredibly complicated (think even more complicated than the brain).
Just to nit-pick and split semantic hairs, but it was certainly the vaccine (and ease of disease identification) that lead to smallpoxes eradication. In that sense the vaccine was 100% effective.
"These preliminary data indicate that the vaccine is 70.4% effective, with tests on two different dose regimens showing that the vaccine was 90% effective if administered at a half dose and then at a full dose, or 62% effective if administered in two full doses."
It is somewhat common to not be sure what is best after phase I/II and so try two different doses. Though normally you try to avoid that because it is more expensive. In this case Oxford thought the two dose was more promising, but the other had enough promise that they start it too just in case. That the second seems better is a surprise, if they expected this result they would have tested differently.
My guess is the lighter dose is really slightly less effective, but the same size is so small that statistical issues make it seem better than it really is.
I wonder what the statistical significance is of those findings. I seems to me that they tried out various different approaches, so the sub-group that received this first-low-second-high treatment might be considerably smaller than the other groups combined leading to slightly less certainty in regards to the findings.
So important:
"A key element of Oxford’s partnership with AstraZeneca is the joint commitment to provide the vaccine on a not-for-profit basis for the duration of the pandemic across the world, and in perpetuity to low- and middle-income countries."
One big difference is that RNA is more generic. Within certain parameters it doesn't matter which specific RNA sequence you produce, it always works the same way and you can use the same facilities for this. There are potential cost advantages there, if you can use a generic, validated process to produce different types of vaccines or drugs without having to develop, tune and certify the core production from scratch every time.
I don't know the economics here, but I would assume that cost advantages are much more likely to appear for small-scale products here than what we have now, producing a billion doses in large factories.
If you're manufacturing something and selling it at a profit, that's absolutely a benefit!
I don't know that the manufacturing costs are less (for Pfizer, Moderna), but I think it's a fair assumption that the bulk of the difference is AstraZeneca (currently) providing it at cost.
My understanding (which might very well be ridiculously wrong) is that mRNA vaccines are a bit like 3d printing; it is incredibly faster and cheaper to build a single one-off item, but if you need to mass produce you still want to go with injection moulding.
Due to the low sample size, it's unclear whether there were no severe cases due to the vaccine -- it's likely that there would have been no severe cases in a given group of 39 COVID-positive individuals even with no intervention.
It depends on the ages of the 39 people. If those were 39 eighty year olds, that would be seriously impressive. If those were 39 twenty year olds it would be expected.
There's no reason to expect that the 39 would have a similar age distribution to the population because it's not a random sample.
Hard to guess. Likely worth investigating, but as secondary priority:
1. You may end up just getting very short and weak immunity, making this approach ineffective.
2. You may get a combination of immunity which can have different efficiency.
3. For some vaccines of same type this works, but is rarely recommended.
4. Mixing partly mRNA and Adenovirus vaccines doesn't to be winning strategy. It is rather more likely to give another vaccine if after two doses you didn't get immunity.
Can you share your thinking around why someone would want to do that given that a combination won't be tested (at-least rigorously). Are you seeing benefits from a logistics point-of-view?
If the vaccines are for the same antigen (eg the spike protein), i would expect that to work fine. Your B cells don't care how the RNA encoding the proteins got into your cells, just what the protein looks like.
A caveat here is that different vaccines might use different versions or modifications of the spike protein, in which case it's possible they wouldn't boost each other. This feels unlikely, though, because i think that would also reduce their effectiveness against the real virus.
I doubt it would help much, for similar reasons why you don't give a flu vaccine to someone already sick.
A vaccine is meant to stimulate adaptive immunity which culminates in formation of memory cells - highly selected T and B lymphocytes which are very specific to the infectious agent.
This process typically takes a couple days [1] and is rather involved. Once you have the memory cells, however, the next time you get in contact with the virus your memory cells will jump-start the immune response much more quickly, before the virus gets a chance to replicate.
In a regular infection the same mechanisms of adaptive immunity are activated, but on top of that you already have the complications from the virus itself (cell death in lung epithelium, accumulation of excess fluid, hypoxia, cytokine storm etc). A vaccine dose won't necessarily speed it up, there are plenty of virus particles already stimulating the immune system - it's just picking up the slack a bit too late.
There are other factors to consider but that's the general idea.
On one hand, all of these vaccine trials excluded people who already had COVID, so we don't fully know what the effect would be in large numbers. However at least one person with COVID immunity accidentally got into the Oxford Phase 1/2 trial (according to earlier published results), so we at least know it didn't hurt them.
On the other hand, it is generally thought that vaccines can trigger immune reactions that are often much stronger and longer lasting than just being infected, so you would expect there to be a benefit to getting vaccinated even if you already had it. But only time will tell for sure. No one really knows how long immunity of either type will last - we just have to wait and find out!
>On the other hand, it is generally thought that vaccines can trigger immune reactions that are often much stronger and longer lasting than just being infected, so you would expect there to be a benefit to getting vaccinated even if you already had it.
How many different viruses are there that cause the common cold? About 200? If we can get an effective vaccine for this coronavirus in under a year why aren't we working on all the other coronaviruses and rhinoviruses? I know nothing about biology but let's say it costs $1 billion to develop and test a successful vaccine for a common cold virus, worldwide for $200 billion that isn't that much to not have to deal with colds anymore. Plus it seems like one vaccine might provide protection for multiple different viruses. Or do they mutate too quickly to keep up?
I would guess that people just don't care enough about getting rid of the common cold. If you're in the vaccine making business, you might as well try and cure some diseases that are killing people. There's more than enough work there already. Also more money...
"There were no hospitalised or severe cases in anyone who received the vaccine"
Does anyone know if there's data for this and the other vaccines, whether any of those that still end up infected under the trials have had any of the secondary symptoms such as missing sense of smell, reduced cognitive function, reduced bio-motor functions, cardiac damage and so on? Not dying from a lung infection is obviously the most important, but some of the other organ damage that corona-virus can cause is pretty scary too, and I'd like to know whether the vaccines seem to prevent this too.
I really still hope mRNA vaccines work well and that we keep investing in them. The potential too rapidly create new vaccines and deploy them when needed without requiring a vector will be crucial to counter future pandemics.
Once the oxford vaccine is deployed I suspect they will then have to create a new vector if they need to create another batch in the future as your body might have developed immunity to the vector virus itself making future doses ineffective.
The whole concept of 'asymptomatic cases' is dubious to begin with, most likely promoted to increase belief in PCR tests and the whole "new normal" environment.
A vaccine is something that primes the immune system, so that when the real virus enters the body it is attacked and destroyed quickly. This means that the virus can never start multiplying in the body and shedding to other people.
I don't believe there is any modern vaccine that doesn't reduce or eliminate asymptomatic spreading of the disease.
However, I believe that it is different between bacteria and viruses.
From my understanding of the whooping cough studies, they found that some vaccinated baboons who were subsequently infected still had high levels of pertussis bacteria after five weeks. These bacteria couldn't cause widespread infections in the host, but had seemingly found pockets where they were safe from the immune system.
A virus, however, can't find a "safe pocket" away from the immune system in which to survive and multiply. It needs to use the body's own cells and machinery to do so, and (outside of the blood-brain barriers) there aren't cells hidden from the immune system.
Note that only n=2,741 people received the 90% efficient dosing. That's 10+ times less than the mRNA vaccines so the confidence intervals on that number will be a lot wider
The 70% is the combined data, so probably the most reliable estimate. For two high doses, they got 62% effectiveness and for one low and one high dose they got 90%. They don't know why the latter was more effective.
70% is still a great effectiveness rate, specially for a cheaper and easier to distribute vaccine.
The problem with adenovirus vaccines is that body might build immunity against the adenovirus as well. So, you give one jab, adenovirus infects enough cells and creates enough antigens, immune systems notices and does something about it, but it also notices the adenovirus and makes antibodies against that, too.
With the second jab those antibodies immediately neutralize the adenovirus so it can't infect enough cells and make enough of the COVID antigens so the protection is not that strong.
The Russian vaccine avoids it by using two different strains of adenovirus for the two jabs
I think they are being very careful because the press will pick every aspect of this to bits and put the worst possible light on any positive spin as in "the secret plot to fool you into taking the failed vaccine developed by Boris Johnson's old university". There will be active attempts to derail any intervention that mitigates the coronavirus crisis because it suits so many bad actors to do that and it suits a large part of the population who like a crisis.
Is that the same vaccine that was approved in Russia? I remember Russia was working with AstraZeneca on their vaccine, but not sure if it's the same one.
No, the Russian one that was released for public use was developed by one of the government institutes (which has a very shady history of falsifying data).
I know it's CNN (what I could find with 5 mins of Googlefu) and they don't explicitly mention the falsified data part. But the Gamaleya Institute is well known in Russia for falsifying data both as a propaganda machine, as well as to obtain further funding from the federal government. I can't find another source I read earlier concerning a past instance of fraud perpetrated by the institute (it was in German).
Does anyone have a pointer on how the mrna vaccine actually works? I understand basic genetics mechanisms and how mrna works inside cells. In shot form, I assume the modified mrna strands are floating through the blood stream. What happens after the injection?
Btw .. I think public health needs to start educating people on how these things work in order to get high coverage. I am alarmed at the number of highly educated people I know who seem suspicious. This fear is just borne by a lack of understanding and can be corrected IMHO.
Thx for the pointer. Yes, I was talking about mrna in the context of the Moderna and Pfizer+B vaccine. This was a good read on why we shouldn't fear reverse transcription. What I still don't get is how free floating mrna molecules in the bloodstream go through the same protein formation process as mrna inside cells. Will continue to search.
The tests are for disease. We hope it protects against infection/the ability to spread it. But that's not part of the testing
I don't know how many existing vaccines fall into either category here, i.e. whether there are many vaccines that prevent disease but do not even reduce the ability to spread. Would be interesting to know.
Obviously we can only say it with high certainty for the duration that the pandemic has been ongoing, but there are strong indications that the immunity will more likely be on the timescale of many years (or even decades)[0]. That effect shouldn't significantly depend on which of the vaccines induced the immunity.
over 7 billion human population, a 90% effectiveness is what? alright? please enlighten me. does anyone know what was the effectiveness of the smallpox vaccine that we did actually manage to eradicate successfully?
The disease will 'die out' (in quotes because it will not actually) if there are not enough targets that are susceptible to it.
People infected by SARS-Cov2 seem to infect two to six other people [0]. Reduce this number by 90% and we are well below one infection per infected, so it is not sustained. This assumes that everyone would be vaccinated.
Currently we are doing something similar: each measure like wearing a mask, social distancing, meeting fewer people, ventilating rooms, finding infected people before they can infect someone else ("contact tracing") contributes to reducing the number of follow-up infections a bit. (This is why "but masks do not really work" is an ill-informed argument. They do not have to because they are meant to be used together with other measures to achieve reduction in spread)
A vaccine will protect us passively instead of requiring us to actively following these measures and will therefore be a lot more convenient.
This is the required immunity of the population, but not the effectiveness of the vaccine. Inside the population there are groups that you cannot put the vaccine (smallest babies, immunosuppressed people, etc).
> One dose of MMR vaccine is 93% effective against measles, 78% effective against mumps, and 97% effective against rubella. Two doses of MMR vaccine are 97% effective against measles and 88% effective against mumps. MMR is an attenuated (weakened) live virus vaccine.
The key point is that if you lower the replication rate-- the number of people each person with the virus goes on to infect-- below 1, the number of active cases exponentially decays to zero.
The business-as-usual replication rate of covid appears to be somewhere around 4-6, meaning that if we have universal vaccination with something like 80% efficacy, the number of active cases will exponentially decay with no other measures taken (social distancing, masks, lockdowns, quarantines etc).
Dr Fauci stated earlier that he was hoping for 70% efficacy. So these results are still good, not just as good as the 94% seen earlier for Moderna's vaccine.
This depends on the r0 of the virus, an r0 of 2 means a 50% effective vaccine (and 100% vaccinated pop) will defeat the virus. With measles and a r0 of 18, youd need an effectiveness of 95%. Considering not everyone can or will take a vaccine, the effectiveness needs to be higher than this.
Covid is apparently around 3, and if you can vaccinate 90% of the population then an effectiveness of 75% would be the minimum you could get away with.
This is if everyone is equally likely to spread the virus.
Probably 20% of people are responsible for 80% of infections. (People who work in shops or public places, people in large extended families, people who socialize a lot).
If you can identify and vaccinate those people it will be much more that 20% effective. (It might be hard to identify those but it's probably easy to identify people at low risk of spreading it and infer)
> We don't need to eradicate it, just get things under control
Based on what we've seen there is no grey area. Either you fully control it which then ends up basically eradicating it e.g. Australia/NZ or you don't and then you end up like EU/US and going in and out of infection waves.
Not really. We haven't (yet?) eradicated the cold or the flu, but we manage to live with them. We need to be able to protect the most vulnerable (probably something like 30% of the population) and reduce load on the healthcare system.
Right now if every activity would be fully available (concerts, conferences, airlines, etc.) every healthcare system across the world would probably be overwhelmed within 2 months, max.
Once we reduce the rates to a trickle, things are probably good enough.
I'm not saying that we shouldn't try to eradicate it, but as with everything, unfortunately, things are frequently taken to a point where they're "good enough" and no further.
In an unvacinated population, yeah, it spreads like wildfire. In a mostly vaccinated population having small pockets, well not good, is not the same level of existential threat. Think about how concerned you are personally about measeles vs how much someone 100 years ago would be.
The thing with the EU is that we have variable, externally controlled infection rates. We could eradicate it, but there's no point because we have land borders to countries we can't control. So we're just trying to keep local rates below crippling. (With mixed success.)
The point of a vaccine is that you can't scale it back for populist appeasement; once you have broad immunity you keep broad immunity for long enough that you end up eradicating the virus almost involuntarily. In comparison, a lockdown is much more vulnerable to feel-good measures reducing the effectiveness.
Eradication means elimination across the entire world. The last 1% is very hard and expensive, requiring sustained funding long after the crisis has passed. To date, we have only managed to eradicate two diseases (smallpox and rinderpest. Not counting diseases that never really managed to spread like SARS) in the entire history of humanity. Ever.
I'm reposting some of my thoughts below to try and genuinely see is someone has an answer to the question:
From a utilitarian perspective, why weren't these all approved for the elderly in Q2 2020?
In other words, its May 2020 and you have the option to ban vaccines or allow vaccines for the elderly, what do you pick?
We know the following about vaccines generally:
-Vaccines have an extremely high success rate, 33% of vaccines make it through all trials to approval. 50% after phase 1 is complete.
-The worst vaccine side effect ever is widely considered to be the swine flu vaccine from 60 years ago, where 1 in 100,000 got GBS, or Pandemrix, where 1 in 18400 got narcolepsy. (1)(2)
-Vaccine candidates have 85% chance of making it from phase III to approved (phase III is supposed to be the efficacy check), in other words we expect about a 15% chance that the vaccine is not effective, most of the tests are about safety.
We know the following about COVID:
-Unknown long term side effects, reasonably likely to be worse than the worst vaccines ever, but unknown.
-The IFR for those over 75 is about 4.6% now(1). Earlier in the pandemic it was about 11.6%(2).
-If you assume that people have a 10% chance of contracting the disease, you can say that those over 75 would have approximately a 0.46% chance of dying (4.6 in 1,000 dead) if they don't get the vaccine. This seems to be a conservative estimate.
So if you have to decide whether to ban a vaccine or not in May 2020, and you assume with 100% confidence that this vaccine was tied for the "worst side effects ever", for example it turns out to be as bad as Pandemrix, then you would expect 1 in 18400 to get something like narcolepsy if you give them the vaccine.
Using the IFR and 10% number above, you assume that not giving the vaccine would leave 84.64 dead for the same population. (85x by volume).
I don't know your opinion of "how much worse is death versus narcolepsy?". If you believe death is 10x worse than narcolepsy, then by severity and volume, taking a vaccine with the worst side effects ever would seem about 850x better than not taking it (in elderly populations). Earlier in the pandemic, when IFRs were over 2x as bad, this was well over 1,000x better.
I mean, the numbers so dramatically favor vaccination that I don't get it at all. Why is this not approved already? Why does it take the FDA 3 weeks to even discuss the matter of approval when this made sense to approve in May? Why did all governments opt to ban the vaccines versus allow them?
While we now get the results from various COVID-19 vaccines I see a societal issue brewing up. How will we deal with the perceived uncertainty of the safety of these vaccines and the surrounding (dis-)infodemic?
I read recently that in some European country (was it Germany?) the willingness to vaccinate against COVID-19 went down from 80% to 60%. With these numbers policy makers will have a hard time convincing the broad population that they can rely on a due process and be safe. In the meantime there is a proliferation of false information and fake news, while in the past there was not much media coverage of significant side effects from a rushed swine flu vaccine [1].
It depends what's more effective: These groups are different: do you jab first those who can most easily spread it, those who would most easily get it or those who would most severely be impacted if they got it.
I think whilst we all want to be safe, ultimately in a year or so, most of the population won't be getting this shot on a regular basis.
For me it's a simple risk proposition, how much at risk do I feel my children or I are from covid. For my children it's a slam dunk; their risk from covid is statistical non existent and weigh that against vaccines that may or may not have long term negative impact on them.
For me, it's not quite so simple as that. I will vaccinate my children, partly to protect them (though the risk to them is low, as you say), but mostly to protect me and my wife, and more importantly our elderly parents. None of the vaccines are 100% effective, and if I can reduce the chances of my kids bringing Covid into the family, I will.
By the time the vaccine is available for my kids, hundreds of millions of people will have already been vaccinated, and there will be very extensive safety data. Part of the requirements for emergency use authorization is extensive monitoring of safety, so if there's any problem with one particular vaccine, it will be known by then.
This issue seems to solve itself. When the risk is higher/more unknown in the early stage, groups that have high/known risk with Covid can take the vaccine. As time passes, more and more data will be gathered on the vaccine risk so the group that can make the correct statistical call to take the vaccine grows. Whether healthy children will take it in 1, 2, 5 or 10 years deepends on what the statistics turn out to be and whether it's required to protect others.
Just to be clear, you have no solid evidence on the long term negative impact on children for either the virus or the vaccine. We have no long term data on anything related to this disease.
But for the deadly virus you interpret the lack sufficient evidence on children as no risk, for the vaccine as as a sign of risk. How do you justify that inconsistency?
>But for the deadly virus you interpret the lack sufficient evidence on children as no risk, for the vaccine as as a sign of risk. How do you justify that inconsistency?
Not the person you're replying to, but looking at similar viruses, there's basically never been a flu-like virus that has no short-term symptoms but serious long-term symptoms, however there have been rushed vaccines that had serious long-term symptoms.
From my perception it’s not that easy. Recently there have been research papers released that estimate long term effects also with children comparable to young adults.
For the sake of argument, let’s assume they are right and that we know that COVID-19 has significant long-term risks for children. How do you outweigh that against the uncertainty of risk of the vaccine?
>> estimate long term effects also with children comparable to young adults
So, like nil then? I still can’t find anything beyond dramatized anecdotes to suggest any special danger beyond what is commensurate with the symptoms.
Just from a software perspective: never install the big version upgrade. Usually the X.0 versions still has bugs that only come out at huge roll outs. I am inclined to wait a few months to let early adaptors test the vaccine.
Medicine is a bit different though and every country probably has institutes checking the vaccines independently. A lot of eyes are on this probably. No company wants to be the company that botched the corona vaccine.
It's likely that the majority of people on HN are not going to be early adopters, and that other groups will get the jab first.
It depends what's more effective, as these groups are all different: do you jab first those who can most easily spread it, those who would most easily get it, those who would most severely be impacted if they got it, or do you jab those who are most diligent, enthusiastic and first in the queue?
I'd even wager that most healthy adults around the world will not be getting the vaccine (but that might be a negative story to run with) but that's at less odds than just healthy, enthusiastic, low risk people getting the jab first.
That option might not be available in the short term. Spain for example aims to vaccinate almost the whole population until summer 2021. What are you going to do when you don’t think it’s version X.1 yet?
I find it disheartening how many people speculate about possible long term side effects of exposure to Covid, even in asymptomatic cases. Yet those same people seemingly have no reservations about injecting a brand new drug into their veins.
It's a simple choice really; being infected with Covid means your body creates thousands of antibodies to fight the virus. Some of those will likely go on and attack your own cells and cause post-covid symptoms. The vaccines only present part of one protein, so not as many antibodies created, less scope for after effects.
Key will be seeing when Pfizer and Moderna release their safety data for their testing cohorts. If the effects are minimal, getting the vaccine is a no-brainer.
Even if you could guarantee that there are no unintended consequences to this drug that was developed over a weekend, which you can't, you must still put a great deal of faith in the motives, incentives, and competence of an entire supply chain.
This is not without risk.
There are a lot of unknowns with this brand new vaccine, yet many of us have personal examples of people in our lives shrugging off a bout of Covid with ease. It's not a completely irrational choice to wait for a few years before taking this vaccine.
That doesn't really make sense. The two things are quite different. How vaccines work and how COVID works are apples and oranges. Do vaccines have potential side effects? Yes. And of course we don't know them. But let's be honest...most of us regular people aren't getting any of these for quite some time. They are going to go to people on the front line and most at risk first.
If you're a front line worker, like a doctor or nurse in a hospital, your chances of getting real COVID with real damage are very high. The long term effects of that are known to be bad. So any long terms effects of the vaccine are more than likely to be way way less dangerous. Also vaccine is, so far, not lethal which makes it a way better option.
Eventually we, the general population, will learn more about these potential side effects of the vaccines and start to gain access to said vaccines. Until then let's not go all anti-vaxxer and pretend we think vaccines give you autism.
> let's not go all anti-vaxxer and pretend we think vaccines give you autism
I agree with most of what you said, but equating rational skepticism with anti-vaxxer paranoia is a bit of a dick move.
Any drug should be approached with great caution, and we should be willing to see its faults even when we're primed to strongly wish for relief from the grip of Covid lockdowns.
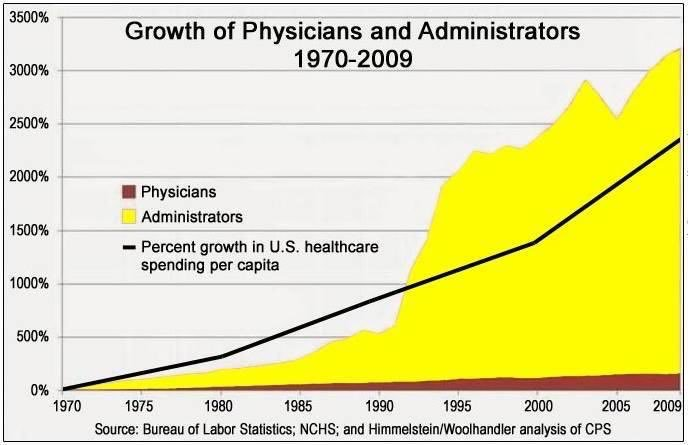{kind=link}
That’s much more accessible to developing / low GDP countries as opposed the cumbersome and expensive storage requirements of the other two.